Math Is Fun Forum
You are not logged in.
- Topics: Active | Unanswered
#2701 2026-02-18 18:16:37
- Jai Ganesh
- Administrator

- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2500) Brain injury/Traumatic Brain Injury
Gist
A Traumatic Brain Injury (TBI) results from an external force—such as a blow, jolt, or penetrating object—causing temporary or permanent damage to brain function, ranging from concussions to severe cognitive, physical, and emotional impairments. Common symptoms include headache, confusion, dizziness, fatigue, and memory loss.
TBIs are sometimes called brain injuries or even head injuries. Some types of TBI can cause temporary or short-term problems with brain function, including problems with how a person thinks, understands, moves, communicates, and acts. More serious TBIs can lead to severe and permanent disability—and even death.
Summary
A traumatic brain injury (TBI) happens when a hit to the head or an object injures your brain. They range from mild to severe and may affect your thinking, movement or emotions. It can cause headaches, confusion or memory loss. Treatment options are available to help you recover.
What Is a Traumatic Brain Injury?
A traumatic brain injury (TBI) happens when an outside force damages your brain and affects how it works. This can occur after a fall, a hard hit to your head, a vehicle accident or when something goes through your skull.
Symptoms can affect your body, thinking and emotions. You may have headaches, confusion, short-term memory loss, and mood or behavior changes. TBIs may be life-threatening. They can cause short-term or long-term health problems that affect many parts of your daily life.
Treatment is available and depends on how serious the injury is.
Types of traumatic brain injuries
There are two types:
* Penetrating TBI: This is when something pierces your skull, enters your brain tissue and damages a part of your brain. Healthcare providers may call these open TBIs.
* Blunt TBI (closed head TBI): This is when something hits your head hard enough that your brain bounces or twists around inside your skull.
What are the severity levels of TBIs?
Healthcare providers classify traumatic brain injuries as being mild, moderate or severe. They may use the term “concussion” when talking about mild TBI. Providers typically group moderate and severe TBIs together.
* Mild TBI: More than 75% of all TBIs are mild. But even mild TBIs may cause significant and long-term issues. For example, you may have trouble returning to your daily routine, including being able to work.
* Moderate and severe TBI: These are medical emergencies. Many develop into significant and long-term health issues.
Details
Brain injury, also known as brain damage or neurotrauma, is the destruction or degeneration of brain cells. It may result from external trauma, such as accidents or falls, or from internal factors, such as strokes, infections, or metabolic disorders.
Traumatic brain injury (TBI), the most common type of brain injury, is typically caused by external physical trauma to the head. Acquired brain injuries occur after birth, in contrast to congenital brain injuries that patients are born with.
In addition, brain injuries can be classified by timing: primary injuries occur at the moment of trauma, while secondary injuries develop afterward due to physiological responses. They can also be categorized by location: focal injuries affect specific areas, whereas diffuse injuries involve widespread brain regions.
The symptoms and complications of brain injuries vary greatly depending on the area(s) of the brain injured, the individual case, the cause of the injury and whether the person receives treatment. People may suffer from headaches, vomit or lose consciousness (potentially falling into a coma or a similar disorder of consciousness) after a brain injury. Long-term cognitive impairment, disturbances in language and motor skills, emotional dysfunction and changes in personality are common.
Treatments for brain injuries include preventing further injuries, medication, physical therapy, psychotherapy, occupational therapy and surgery. Because of neuroplasticity, the brain can partially recover function by forming new neural connections to compensate for damaged areas. Patients may regain adaptive skills such as movement and speech, especially if they undergo therapy and practice.
Classification:
Focal and diffuse
Focal brain injuries affect only a single area of the brain; they result from direct force to the head[4] and manifest as haemorrhages, contusions, and subdural and epidural haematomas. Diffuse brain injuries cause widespread damage to all or many areas, and are caused by diffuse axonal injuries, hypoxia, ischaemia and vascular injuries. If both are severe, focal brain injuries are deadlier than diffuse ones; severe focal and diffuse injuries have mortality rates of 40% and 25% respectively. Although, diffuse brain injuries more often result in long-term neurological and cognitive deficits.
Primary and secondary
Primary brain injuries, most of which are traumatic brain injuries, occur directly because of mechanical forces that deform the brain. Secondary brain injuries result from conditions, such as hypoxia, ischaemia, oedema, hydrocephalus and intracranial hypertension, that may or may not be the aftereffects of primary brain injuries.
Signs and symptoms
Symptoms of brain injuries vary based on the severity of the injury, the area of the brain injured, and how much of the brain was affected. The three categories used for classifying the severity of brain injuries are mild, moderate and severe.
Severity of injuries:
Mild brain injuries
When caused by a blow to the head, a mild brain injury is known as a concussion. Symptoms of a mild brain injury include headaches, confusion, tinnitus, fatigue and changes in sleep patterns, mood or behavior. Other symptoms include trouble with memory, concentration, attention or thinking. Because mental fatigue can be attributed to many disorders, patients may not realise the connection between fatigue and a minor brain injury.
Moderate/severe brain injuries
Cognitive symptoms include confusion, aggression, abnormal behavior and slurred speech. Physical symptoms include a loss of consciousness, headaches that worsen or do not go away, vomiting or nausea, convulsions, brain pulsation, abnormal dilation of the eyes, inability to wake from sleep, weakness in extremities and a loss of coordination.
Symptoms in children
Young children could be unable to communicate their physical states, emotions and thought processes, so parents, physicians and caregivers may need to observe their behaviours to discern symptoms. Signs include changes in eating habits, persistent anger, sadness, attention loss, losing interest in activities they used to enjoy, or sleep problems.
Complications:
Physiological effects
Physiological complications of a brain injury, caused by damage to the neurons, nerve tracts or sections of the brain, can occur immediately or at varying times after the injury. The immediate response can take many forms. Initially, there may be symptoms such as swelling, pain, bruising, or loss of consciousness. Headaches, dizziness and fatigue, which can develop as time progresses, may become permanent or persist for a long time.
Brain damage predisposes patients to seizures, Parkinson's disease, dementia and hormone-secreting gland disorders; monitoring is essential for detecting the development of these diseases and treating them promptly.
Diffuse brain injuries, brain injuries that result in intracranial hypertension and brain injuries affecting parts of the brain responsible for consciousness may induce a coma, a prolonged period of deep unconsciousness. Severe brain injuries may cause a persistent vegetative state in which a patient displays wakefulness without any awareness of his or her surroundings.
Brain death occurs when all activity of the brain is deemed to have irreversibly ceased. The prerequisite for considering brain death is the presence of an injury, bodily status (e.g. hyperpyrexia) or disease that has severely damaged the entire brain. After this has been confirmed, the criteria for ascertaining brain death are an absence of brain activity 24 hours after a patient has been resuscitated, an absence of brainstem reflexes (including the pupillary response and gag reflex) and an absence of spontaneous breathing when the lungs are filled with carbon dioxide.
Cognitive effects
Post-traumatic amnesia, and issues with both long- and short-term memory, are common with brain damage, as is temporary aphasia, or impairment of language. Tissue damage and loss of blood flow caused by the injury may cause both of these issues to become permanent. Apraxia, the impairment of motor coordination and movement, has also been documented.
Cognitive effects can depend on the location of the brain that was damaged, and certain types of impairments can be attributed to damage to certain areas of the brain. Larger lesions tend to cause worse symptoms and more complicated recoveries.
Brain lesions in Wernicke's and Broca's areas are correlated with language, speech and category-specific disorders. Wernicke's aphasia is associated with word retrieval deficits, unknowingly making up words (neologisms), and problems with language comprehension. The symptoms of Wernicke's aphasia are caused by damage to the posterior section of the superior temporal gyrus.
Damage to Broca's area typically produces symptoms like omitting functional words (agrammatism), sound production changes, alexia, agraphia, and problems with comprehension and production. Broca's aphasia is indicative of damage to the posterior inferior frontal gyrus of the brain.
The impairment of a cognitive process following a brain injury does not necessarily indicate that the damaged area is wholly responsible for the process that is impaired. For example, in pure alexia, the ability to read is destroyed by a lesion damaging both the left visual field and the connection between the right visual field and the language areas (Broca's area and Wernicke's area). However, this does not mean one with pure alexia is incapable of comprehending speech—merely that there is no connection between their working visual cortex and language areas—as is demonstrated by the fact that people with pure alexia can still write, speak, and even transcribe letters without understanding their meaning.
Lesions to the fusiform gyrus often result in prosopagnosia, the inability to distinguish faces and other complex objects from each other. Lesions in the amygdala would eliminate the enhanced activation seen in occipital and fusiform visual areas in response to fear with the area intact. Amygdala lesions change the functional pattern of activation to emotional stimuli in regions that are distant from the amygdala.
Other lesions to the visual cortex have different effects depending on the location of the damage. Lesions to V1, for example, can cause blindsight in different areas of the brain depending on the size of the lesion and location relative to the calcarine fissure. Lesions to V4 can cause color-blindness, and bilateral lesions to MT/V5 can cause the loss of the ability to perceive motion. Lesions to the parietal lobes may result in agnosia, an inability to recognize complex objects, smells, or shapes, or amorphosynthesis, a loss of perception on the opposite side of the body.
Psychological effects
There are documented cases of lasting psychological effects as well, such as emotional changes often caused by damage to the various parts of the brain that control emotions and behaviour. Individuals may experience sudden, severe mood swings that subside quickly. Emotional changes, which may not be triggered by a specific event, can cause distress to the injured party and their family and friends. Brain injuries increase the risk of developing depression, bipolar disorder and schizophrenia. The more severe a brain injury is the likelier it is to cause bipolar disorder or schizophrenia; the correlation between brain injuries and mental illness is stronger in female and older patients. Often, counseling in either a one-on-one or group setting is suggested for those who experience emotional dysfunction after their injury.
Any type of acquired brain injury can result in changes in personality, including, with regards to the Big Five personality traits, increased neuroticism, decreased extraversion and decreased conscientiousness. If the patient is aware of the change in his or her cognitive capacity, personality and mental state after an injury, he or she might feel disconnected from his or her pre-injury identity, leading to irritability, emotional distress and a disrupted concept of self.
Additional Information
Traumatic brain injury (TBI) happens when a sudden, external, physical assault damages the brain. It is one of the most common causes of disability and death in adults. TBI is a broad term that describes a vast array of injuries that happen to the brain. The damage can be focal (confined to one area of the brain) or diffuse (happens in more than one area of the brain). The severity of a brain injury can range from a mild concussion to a severe injury that results in coma or even death.
What are the different types of TBI?
Brain injury may happen in one of two ways:
* Closed brain injury. Closed brain injuries happen when there is a nonpenetrating injury to the brain with no break in the skull. A closed brain injury is caused by a rapid forward or backward movement and shaking of the brain inside the bony skull that results in bruising and tearing of brain tissue and blood vessels. Closed brain injuries are usually caused by car accidents, falls, and increasingly, in sports. Shaking a baby can also result in this type of injury (called shaken baby syndrome).
* Penetrating brain injury. Penetrating, or open head injuries happen when there is a break in the skull, such as when a bullet pierces the brain.
What is diffuse axonal injury (DAI)?
Diffuse axonal injury is the shearing (tearing) of the brain's long connecting nerve fibers (axons) that happens when the brain is injured as it shifts and rotates inside the bony skull. DAI usually causes coma and injury to many different parts of the brain. The changes in the brain are often microscopic and may not be evident on computed tomography (CT scan) or magnetic resonance imaging (MRI) scans.
What is primary and secondary brain injury?
Primary brain injury refers to the sudden and profound injury to the brain that is considered to be more or less complete at the time of impact. This happens at the time of the car accident, gunshot wound, or fall.
Secondary brain injury refers to the changes that evolve over a period of hours to days after the primary brain injury. It includes an entire series of steps or stages of cellular, chemical, tissue, or blood vessel changes in the brain that contribute to further destruction of brain tissue.
What causes a head injury?
There are many causes of head injury in children and adults. The most common injuries are from motor vehicle accidents (where the person is either riding in the car or is struck as a pedestrian), violence, falls, or as a result of shaking a child (as seen in cases of child abuse).
What causes bruising and internal damage to the brain?
When there is a direct blow to the head, the bruising of the brain and the damage to the internal tissue and blood vessels is due to a mechanism called coup-contrecoup. A bruise directly related to trauma at the site of impact is called a coup lesion (pronounced COO). As the brain jolts backward, it can hit the skull on the opposite side and cause a bruise called a contrecoup lesion. The jarring of the brain against the sides of the skull can cause shearing (tearing) of the internal lining, tissues, and blood vessels leading to internal bleeding, bruising, or swelling of the brain.
What are the possible results of brain injury?
Some brain injuries are mild, with symptoms disappearing over time with proper attention. Others are more severe and may result in permanent disability. The long-term or permanent results of brain injury may need post-injury and possibly lifelong rehabilitation. Effects of brain injury may include:
* Cognitive deficits
** Coma
** Confusion
** Shortened attention span
** Memory problems and amnesia
** Problem-solving deficits
** Problems with judgment
** Inability to understand abstract concepts
** Loss of sense of time and space
** Decreased awareness of self and others
** Inability to accept more than one- or two-step commands at the same time
* Motor deficits
** Paralysis or weakness
** Spasticity (tightening and shortening of the muscles)
** Poor balance
** Decreased endurance
** Inability to plan motor movements
** Delays in getting started
** Tremors
** Swallowing problems
** Poor coordination
* Perceptual or sensory deficits
** Changes in hearing, vision, taste, smell, and touch
** Loss of sensation or heightened sensation of body parts
** Left- or right-sided neglect
** Difficulty understanding where limbs are in relation to the body
** Vision problems, including double vision, lack of visual acuity, or limited range of vision
* Communication and language deficits
** Difficulty speaking and understanding speech (aphasia)
** Difficulty choosing the right words to say (aphasia)
** Difficulty reading (alexia) or writing (agraphia)
** Difficulty knowing how to perform certain very common actions, like brushing one's teeth (apraxia)
** Slow, hesitant speech and decreased vocabulary
** Difficulty forming sentences that make sense
** Problems identifying objects and their function
** Problems with reading, writing, and ability to work with numbers
* Functional deficits
** Impaired ability with activities of daily living (ADLs), such as dressing, bathing, and eating
** Problems with organization, shopping, or paying bills
** Inability to drive a car or operate machinery
* Social difficulties
** Impaired social capacity resulting in difficult interpersonal relationships
** Difficulties in making and keeping friends
** Difficulties understanding and responding to the nuances of social interaction
* Regulatory disturbances
** Fatigue
** Changes in sleep patterns and eating habits
** Dizziness
** Headache
** Loss of bowel and bladder control
* Personality or psychiatric changes
** Apathy
** Decreased motivation
** Emotional lability
** Irritability
** Anxiety and depression
** Disinhibition, including temper flare-ups, aggression, cursing, lowered frustration tolerance, and inappropriate sexual behavior
Certain psychiatric disorders are more likely to develop if damage changes the chemical composition of the brain.
* Traumatic Epilepsy
** Epilepsy can happen with a brain injury, but more commonly with severe or penetrating injuries. While most seizures happen immediately after the injury, or within the first year, it is also possible for epilepsy to surface years later. Epilepsy includes both major or generalized seizures and minor or partial seizures.
Can the brain heal after being injured?
Most studies suggest that once brain cells are destroyed or damaged, for the most part, they do not regenerate. However, recovery after brain injury can take place, especially in younger people, as, in some cases, other areas of the brain make up for the injured tissue. In other cases, the brain learns to reroute information and function around the damaged areas. The exact amount of recovery is not predictable at the time of injury and may be unknown for months or even years. Each brain injury and rate of recovery is unique. Recovery from a severe brain injury often involves a prolonged or lifelong process of treatment and rehabilitation.
What is coma?
Coma is an altered state of consciousness that may be very deep (unconsciousness) so that no amount of stimulation will cause the patient to respond. It can also be a state of reduced consciousness, so that the patient may move about or respond to pain. Not all patients with brain injury are comatose. The depth of coma, and the time a patient spends in a coma varies greatly depending on the location and severity of the brain injury. Some patients emerge from a coma and have a good recovery. Other patients have significant disabilities.
How is coma measured?
Depth of the coma is usually measured in the emergency and intensive care settings using a Glasgow coma scale. The scale (from 3 to 15) evaluates eye opening, verbal response, and motor response. A high score shows a greater amount of consciousness and awareness.
In rehabilitation settings, here are several scales and measures used to rate and record the progress of the patient. Some of the most common of these scales are described below.
* Rancho Los Amigos 10 Level Scale of Cognitive Functioning. This is a revision of the original Rancho 8 Level Scale, which is based on how the patient reacts to external stimuli and the environment. The scales consist of 10 different levels and each patient will progress through the levels with starts and stops, progress and plateaus.
* Disability Rating Scale (DRS). This scale measures functional change during the course of recovery rating the person's disability level from none to extreme. The DRS assesses cognitive and physical function, impairment, disability, and handicap and can track a person's progress from "coma to community."
* Functional Independent Measure (FIM). The FIM scale measures a person's level of independence in activities of daily living. Scores can range from 1 (complete dependence) to 7 (complete independence).
* Functional Assessment Measure (FAM). This measure is used along with FIM and was developed specifically for people with brain injury.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2702 2026-02-20 22:08:25
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2501) Sweden - The Country With Most Number Of Islands In The World
Gist
Sweden boasts a total of 267,570 islands. "Sweden has more islands than any other country in the world, and we would like to invite people to enjoy what may be the most genuine form of luxury: the peace and tranquillity of nature on your own island", says Susanne Andersson, CEO at Visit Sweden.
Sweden has the highest number of islands of any country in the world, with a total of 267,570. The vast majority of these are uninhabited, with fewer than 1,000 having permanent residents. The Stockholm archipelago alone features nearly 30,000 islands and skerries.
Interestingly, when it comes to statistics regarding which countries have the most islands, figures can differ hugely between sources. Pulling together the most reputable and official sources it could, website worldatlas.com has found that out of all countries on the planet, Sweden has the most islands with 267,570, the majority of which are uninhabited. Even the capital of Stockholm is built across a 14-island archipelago with more than 50 bridges.
Summary
Sweden, formally the Kingdom of Sweden, is a Nordic country located on the Scandinavian Peninsula in Northern Europe. It borders Norway to the west and north, and Finland to the east. At 450,295 square kilometres (173,860 sq mi), Sweden is the largest Nordic country by both area and population, and is the fifth-largest country in Europe. Its capital and largest city is Stockholm. Sweden has a population of 10.6 million, and a low population density of 25.5 inhabitants per square kilometre (66/sq mi); 88% of Swedes reside in urban areas. They are mostly in the central and southern half of the country. Sweden's urban areas together cover 1.5% of its land area. Sweden has a diverse climate owing to the length of the country, which ranges from 55°N to 69°N.
Sweden has been inhabited since prehistoric times around 12,000 BC. The inhabitants emerged as the Geats (Swedish: Götar) and Swedes (Svear), who formed part of the sea-faring peoples known as the Norsemen. A unified Swedish state was established during the late 10th century. In 1397, Sweden joined Norway and Denmark to form the Scandinavian Kalmar Union, which Sweden left in 1523. When Sweden became involved in the Thirty Years' War on the Protestant side, an expansion of its territories began, forming the Swedish Empire, which remained one of the great powers of Europe until the early 18th century. During this era Sweden controlled much of the Baltic Sea. Most of the conquered territories outside the Scandinavian Peninsula were lost during the 18th and 19th centuries. The eastern half of Sweden, present-day Finland, was lost to Imperial Russia in 1809. The last war in which Sweden was directly involved was in 1814, when Sweden by military means forced Norway into a personal union, a union which lasted until 1905.
Sweden is a highly developed country ranked fifth in the Human Development Index. It is a constitutional monarchy and a parliamentary democracy, with legislative power vested in the 349-member unicameral Riksdag. It is a unitary state, divided into 21 counties and 290 municipalities. Sweden maintains a Nordic social welfare system that provides universal health care and tertiary education for its citizens. It has the world's 14th highest GDP per capita and ranks very highly in quality of life, health, education, protection of civil liberties, economic competitiveness, income equality, gender equality and prosperity. Sweden joined the European Union on 1 January 1995 and NATO on 7 March 2024. It is also a member of the United Nations, the Schengen Area, the Council of Europe, the Nordic Council, the World Trade Organization and the Organisation for Economic Co-operation and Development (OECD).
Details
Sweden is a country located on the Scandinavian Peninsula in northern Europe. The name Sweden was derived from the Svear, or Suiones, a people mentioned as early as 98 ce by the Roman author Tacitus. The country’s ancient name was Svithiod. Stockholm has been the permanent capital since 1523.
Sweden occupies the greater part of the Scandinavian Peninsula, which it shares with Norway. The land slopes gently from the high mountains along the Norwegian frontier eastward to the Baltic Sea. Geologically, it is one of the oldest and most stable parts of the Earth’s crust. Its surface formations and soils were altered by the receding glaciers of the Pleistocene Epoch (about 2,600,000 to 11,700 years ago). Lakes dot the fairly flat landscape, and thousands of islands form archipelagoes along more than 1,300 miles (2,100 km) of jagged, rocky coastline. Like all of northwestern Europe, Sweden has a generally favourable climate relative to its northerly latitude owing to moderate southwesterly winds and the warm North Atlantic Current.
The country has a 1,000-year-long continuous history as a sovereign state, but its territorial expanse changed often until 1809. Today it is a constitutional monarchy with a well-established parliamentary democracy that dates from 1917. Swedish society is ethnically and religiously very homogeneous, although recent immigration has created some social diversity. Historically, Sweden rose from backwardness and poverty into a highly developed postindustrial society and advanced welfare state with a standard of living and life expectancy that rank among the highest in the world.
Sweden long ago disavowed the military aggressiveness that once involved its armies deeply in Europe’s centuries of dynastic warfare. It has chosen instead to play a balancing role among the world’s conflicting ideological and political systems. It is for this reason that Swedish statesmen have often been sought out to fill major positions in the United Nations. At peace since 1814, Sweden has followed the doctrine, enunciated in every document on foreign policy since World War II, of “nonalignment in peace aiming at neutrality in war.”
Land
Sweden lies to the southwest of Finland. A long coastline forms the country’s eastern border, extending along the Gulf of Bothnia and the Baltic Sea; a narrow strait, known as The Sound (Öresund), separates Sweden from Denmark in the south. A shorter coastline along the Skagerrak and Kattegat straits forms Sweden’s border to the southwest, and Norway lies to the west. Sweden extends some 1,000 miles (1,600 km) to the north and south and 310 miles (500 km) to the east and west.
The country is traditionally divided into three regions: to the north is Norrland, the vast mountain and forest region; in central Sweden is Svealand, an expanse of lowland in the east and highland in the west; and in the south is Götaland, which includes the Småland highlands and, at the southern extremity, the small but rich plains of Skåne. In the far north the region of Lappland overlaps Norrland and northern Finland.
Relief
Norrland is the largest and most sparsely populated of the regions, covering some three-fifths of the country. The region features an undulating surface of rounded hills and mountains, large lakes, and extensive river valleys. To the west lie the Kölen (Kjølen; Scandinavian) Mountains, through which runs the border demarcating Sweden and Norway. This range is characterized by numerous glaciers, the southernmost of which is on Helags Mountain (Helagsfjället), near the Norwegian border. At the region’s far northern edge, north of the Arctic Circle, are Sweden’s highest peaks: Mount Kebne (Kebnekaise), which is 6,926 feet (2,111 metres) in elevation, and Mount Sarek (Sarektjåkkå), which rises 6,854 feet (2,089 metres), in the magnificent Sarek National Park.
The interior of southern Sweden, Småland, is a wooded upland with elevations of 980 to 1,300 feet (300 to 400 metres). A region of poor and stony soils, Småland has been cultivated through the ages with some difficulty, as evidenced by the enormous mounds of stone cleared from the land. More recently the area has been characterized by flourishing small factories.
Except for a stretch of scenic “high coast,” the Bothnian coastal plain is low-lying and stretches from Norrland into Svealand. Most of the fairly level surface of eastern Svealand and northern Götaland was pressed below sea level by glaciers, leaving a landscape of fragmented bedrock, fertile clayey plains, numerous lakes, and sandy ridges. Today these are intermingled with mixed forests and farmland. Sweden’s landscape changes from the hills of Småland to the fertile plains of Skåne, which is physiographically and economically more similar to Denmark than to the rest of Sweden. This is Sweden’s oldest settled and most densely populated agricultural area.
The Swedish coastline is typically rocky, with hundreds of small, sometimes wooded islands. Ground by glacial ice in the same direction, they have a common rounded shape. This type of coast, known as skärgård, is found in both the east and the west, especially around Stockholm and Gothenburg. Off the southern coast in the Baltic, the large, flat islands of Öland and Gotland are outcropping layers of sandstone and limestone.
Drainage
The country’s chief rivers originate in the mountains of Norrland, mostly flowing southeastward with many falls and rapids and emptying into the Gulf of Bothnia or the Baltic Sea. The longest, however, is the Klar-Göta River, which rises in Norway and flows 447 miles (719 km), reaching Lake Väner (Vänern) and continuing southward out of the lake’s southern end to the North Sea; along its southernmost course are the famous falls of Trollhättan. The Muonio and Torne rivers form the frontier with Finland, and in the south the Dal River marks the transition to Svealand. The rivers, except in the far north, where they are protected, are sources of hydroelectric power.
In Svealand are Sweden’s largest lakes, including Lakes Väner, 2,181 square miles (5,650 square km); Vätter (Vättern), 738 square miles (1,911 square km); and Mälar (Mälaren), 440 square miles (1,139 square km). The shores of Lakes Siljan and Storsjön and the river valleys support agriculture.
Soils
The dominant soil of Sweden is till, formed under glacial ice. Till that comes from the archaic bedrock of granites and gneisses forms a poor soil, and forestry and polluted (acid) rain add to its acidification. On the other hand, small areas of clayey till from younger sedimentary limestone, scattered mainly in southern Sweden, form brown earth, providing agricultural soils of high fertility. In addition, vast areas of central Sweden are covered by heavy and fertile sea-bottom clays raised out of the sea by postglacial land uplift. One-fifth of the country, especially in rainy southwestern Sweden and the cold far north, is covered by marshland and peat.
Climate of Sweden
About 15 percent of the country lies within the Arctic Circle. From about late May until mid-July, sunlight lasts around the clock north of the Arctic Circle, but, even as far south as Stockholm, the nights during this period have only a few hours of semidarkness. In mid-December, on the other hand, Stockholm experiences only about 5.5 hours of daylight; in areas as far north as Lappland, there are nearly 20 hours of total darkness relieved by a mere 4 hours of twilight.
Considering its northerly geographic location (at the latitude of parts of Greenland and Siberia), Sweden enjoys a favourable climate. From the southwest, Atlantic low-pressure winds blow in air warmed by the North Atlantic Current and make the weather mild but changeable. Another type of influence comes from continental high pressures to the east. These create sunny weather, which is hot in summer and cold in winter. The interaction between the Atlantic and continental influences causes periodic shifts in climate.
The north-to-south extension of the country and the higher elevation of the northern part results in great regional differences in winter climate. The northern interior receives heavy snowfall for up to eight months of the year and has severe temperatures that drop as low as −22 to −40 °F (−30 to −40 °C). The average January temperature in Haparanda at the head of the Gulf of Bothnia is 10 °F (−12 °C). Sea ice covers the Gulf of Bothnia from November to May.
In southern Sweden winters vary more from year to year than in the north; snowfall is irregular, and average January temperatures range between 23 and 32 °F (−5 and 0 °C). Coastal waters seldom freeze.
Summer temperatures vary far less, although summer is much shorter in the north. In terms of average daily temperature, “spring” arrives in Skåne during February but not until late May in northernmost Norrland; then it may come virtually overnight. The mean July temperature in Haparanda is 59 °F (15 °C), and in Malmö 63 °F (17 °C).
Late summer and autumn are the rainiest seasons, but precipitation falls throughout the year. Annual precipitation averages about 24 inches (600 mm).
Plant and animal life
Most of Sweden is dominated by forests of fir, pine, and birch. Southern Sweden has more mixed forests, and in the far south deciduous trees such as beech, oak, linden, ash, elm, and maple are common. The forests are rich in berries, lingonberries and blueberries among them, and mushrooms. In Sweden anyone is entitled to hike through the forests and fields and pick berries and mushrooms.
In the high mountains coniferous trees give way to mountain birches, which extend up to the tree line at an elevation of 1,600 to 2,900 feet (480 to 880 metres). The treeless mountains with their heaths, marshes, and boulder fields have Alpine flora. Dwarf birch and willows are typical.
Owing to their limestone bedrock and mild climate, Gotland and Öland have a special flora that includes many orchids.
Bears and lynx still inhabit the northern forests, while wolves are making a comeback, having become almost completely extinct in the 20th century. Throughout the country are large numbers of moose, roe deer, foxes, and hares. The moose is a great prize for hunters, but it also constitutes a traffic hazard. Hunting and fishing are closely regulated, and many species of animals are fully protected. Large herds of domesticated reindeer owned by Sami (Lapps) graze the northern mountains and forests.
Winter birdlife is dominated by a few species, but summer brings large numbers of migratory birds from southern Europe and Africa, as, for example, cranes and wild geese. Sweden has a rich variety of aquatic animal life, but environmental pollution has taken its toll. This applies significantly to the Baltic seal. Fish species include the cod and mackerel of the deep, salty Atlantic and the salmon and pike found in the far less saline Baltic and in lakes and rivers. Atlantic herring and its smaller relative, the Baltic herring, are traditional staple foods.
Conservation
Sweden has been in the vanguard of countries seeking to preserve the natural environment. It was the first European country to establish a national park (Sarek National Park was established in 1909), thereby preserving part of Europe’s last wilderness. The first Nature Conservancy Act was adopted in 1909, and in 1969 a modern environmental protection act was passed. Since then tens of thousands of square miles have been set aside as national parks and nature reserves. Serious environmental problems persist nevertheless. About one-fifth of the lakes in Sweden have been damaged by acidification, and groundwater too is threatened. A chief cause is sulfur fallout (i.e., contamination by what is commonly known as acid rain); most of the sulfur is discharged into the atmosphere by industrial facilities in nearby countries. Pollution in the Baltic Sea and the coastal waters of the Kattegat and Skagerrak also is considered severe.
People:
Ethnic groups
Although different groups of immigrants have influenced Swedish culture through the centuries, the population historically has been unusually homogeneous in ethnic stock, language, and religion. It is only since World War II that notable change has occurred in the ethnic pattern. From 1970 to the early 1990s, net immigration accounted for about three-fourths of the population growth. By far, most of the immigrants came from the neighbouring Nordic countries, with which Sweden shares a common labour market.
In the 1980s Sweden began to receive an increasing number of asylum seekers from Asian and African countries such as Iran, Iraq, Lebanon, Turkey, Eritrea, and Somalia, as well as from Latin American countries that were suffering under repressive governments. Then from 2010 to 2014 the number of people seeking asylum in Sweden expanded dramatically, reaching more than 80,000 in 2014, and that number doubled to more than 160,000 in 2015. Many of these people were fleeing the Syrian Civil War. From the beginning of that conflict, Sweden had granted residency to any Syrian seeking asylum (some 70,000 in total). Thus, by 2016 one in six Swedish residents had been born outside the country, and Sweden, feeling the strain of the mass influx of migrants, enacted new and more stringent immigration restrictions.
Sweden has two minority groups of indigenous inhabitants: the Finnish-speaking people of the northeast along the Finnish border, and the Sami (Lapp) population of about 15,000 scattered throughout the northern Swedish interior. Once a hunting and fishing people, the latter group developed a reindeer-herding system that they still operate. Most of the Sami in Sweden have other occupations as well.
Languages
Swedish, the national language of Sweden and the mother tongue of approximately nine-tenths of the population, is a Nordic language. It belongs to the North Germanic (Scandinavian) subgroup of the Germanic languages and is closely related to the Danish, Norwegian, Icelandic, and Faeroese languages. It has been influenced at times by German, but it has also borrowed some words and syntax from French, English, and Finnish. A common standard language (rikssvenska) has been in use more than 100 years. The traditionally varying dialects of the provinces, although homogenized rapidly through the influences of education and the mass media, are still widely spoken. Swedish is also spoken by about 300,000 Finland-Swedes. Swedish law recognizes Sami and Finnish (both of which belong to the Uralic language group), as well as Meänkieli (the Finnish of the Torne Valley), Romani, and Yiddish as national minority languages, along with sign language. About 200 languages are now spoken in Sweden, owing to immigrants and refugees.
Religion of Sweden
Prehistoric archaeological artifacts and sites—including graves and rock carvings—give an indication of the ancient system of religious beliefs practiced in Sweden during the pre-Christian era. The sun and seasons figured largely, in tandem with fertility rites meant to ensure good harvests. These practices were informed by a highly developed mythic cycle, describing a distinctive cosmology and the deeds of the Old Norse gods, giants, and demons. Important gods included Odin, Thor, Freyr, and Freyja. Great sacrificial rites, thought to have taken place every eight years at Old Uppsala, were described by the author Adam of Bremen in the 11th century.
Sweden adopted Christianity in the 11th century, and for nearly 500 years Roman Catholicism was the preeminent religion. Sweden was the home to St. Bridget, founder of the Brigittine convent at Vadstena. As the first waves of the Protestant Reformation swept Europe in the mid-1500s, Lutheranism took hold in Sweden and remained dominant. The Evangelical Lutheran Church of Sweden was the official state church until 2000, and between three-fifths and two-thirds of the population remains members of this church. Since the late 1800s a number of independent churches have emerged; however, their members can also belong to the Church of Sweden. Immigration has brought a steady increase to the membership of the Roman Catholic, Greek Orthodox, and Islamic religions. Judaism is the country’s oldest global non-Christian religion, practiced in Sweden since 1776. After Christianity, Islam is the largest religion in Sweden, with about 100,000 active practitioners at the turn of the 21st century, although the number of Swedes of Muslim heritage was nearly three times that number.
Additional Information
Sweden is in the geographical region known as Scandinavia in northern Europe.
Sweden is in the geographical region known as Scandinavia in northern Europe. Lush, large forests cover half of the country and over 100,000 lakes dot the landscape. The lakes, and over 24,000 islands, are all open to the public through Sweden's tradition of right to public access.
Sweden is 977 miles (1,572 kilometers) long and is bordered by Norway on the west and Finland to the east. Three stretches of water separate Sweden from Denmark—the Skagerrak, the Kattegat, and the Öresund straits.
Sweden's Arctic north has been called the "land of the midnight sun," because during the summer months the sun never sets. Even in the capital of Stockholm in the south, the summer nights last only four hours and the sky doesn't deepen beyond twilight. But winter lasts until May and the nights are long and the days are short.
In the fall and spring, there are spectacular light shows in northern Sweden known as the "aurora borealis," or "northern lights." The dazzling green or red lights, which fill the late night sky, are caused by collisions of tiny particles high in the Earth's atmosphere.
People and Cultre
Sweden is one of the least populated countries in Europe, with a population of less than 10 million people. Most people used to live in the countryside, but as the country became industrialized in the 1900s, many moved to the cities of Malmö, Göteborg, and Stockholm.
During the 1930s, Sweden developed the welfare system, known as "the Swedish model." Under their system, all Swedes have access to publicly financed health care, help for the unemployed, child care, schools, elder care, and at least five weeks of paid vacation per year.
Nature
Ancient forests, broadleaved woodlands, mountains, and wetlands provide rich habitats for many endangered animals and birds. Swedes love the countryside and Sweden was the first country in Europe to create national parks. Today, there are 29 national parks and many nature reserves and wildlife sanctuaries.
Sweden is the center of an effort to save the critically endangered arctic fox, which is on the brink of extinction with fewer than 200 left in Europe. During the winter months, their fur turns from brown to white to match the snowy landscape. The northern forests are home to brown bears and wolverines, which are related to badgers and otters, not wolves.
Carl Von Linne, known as Carolus Linnaeus, was a well-known Swedish botanist, born in the 1700s. Linnaeus invented the method for naming plants and animals which is used today. Every living thing has a Latin name that is divided into two parts. The first part gives its group, or genus, and the second part of the name gives its kind, or species.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2703 2026-02-22 17:31:14
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2502) Maglev Train
Gist
Maglev (magnetic levitation) trains are high-speed vehicles that use electromagnetic forces to float, guide, and propel themselves 10 cm (approx. 4 inches) above a guideway instead of using wheels, axles, or traditional engines. By eliminating friction, they achieve speeds exceeding 600 km/h (373 mph), offering a quiet, low-maintenance, and energy-efficient alternative to traditional rail.
Maglev trains are significantly faster than traditional bullet trains because they use magnetic levitation to float above the tracks, eliminating friction and allowing for much higher speeds, with operational speeds over 500 km/h compared to bullet trains' 320 km/h, and test records exceeding 600 km/h.
Summary
Maglev is a a floating vehicle for land transportation that is supported by either electromagnetic attraction or repulsion. Maglevs were conceptualized during the early 1900s by American professor and inventor Robert Goddard and French-born American engineer Emile Bachelet and have been in commercial use since 1984, with several operating at present and extensive networks proposed for the future.
Maglevs incorporate a basic fact about magnetic forces—like magnetic poles repel each other, and opposite magnetic poles attract each other—to lift, propel, and guide a vehicle over a track (or guideway). Maglev propulsion and levitation may involve the use of superconducting materials, electromagnets, diamagnets, and rare-earth magnets.
Electromagnetic suspension (EMS) and electrodynamic suspension (EDS)
Two types of maglevs are in service. Electromagnetic suspension (EMS) uses the attractive force between magnets present on the train’s sides and underside and on the guideway to levitate the train. A variation on EMS, called Transrapid, employs an electromagnet to lift the train off the guideway. The attraction from magnets present on the underside of the vehicle that wrap around the iron rails of the guideway keep the train about 1.3 cm (0.5 inch) above the guideway.
Electrodynamic suspension (EDS) systems are similar to EMS in several respects, but the magnets are used to repel the train from the guideway rather than attract them. These magnets are supercooled and superconducting and have the ability to conduct electricity for a short time after power has been cut. (In EMS systems a loss of power shuts down the electromagnets.) Also, unlike EMS, the charge of the magnetized coils of the guideway in EDS systems repels the charge of magnets on the undercarriage of the train so that it levitates higher (typically in the range of 1–10 cm [0.4–3.9 inches]) above the guideway. EDS trains are slow to lift off, so they have wheels that must be deployed below approximately 100 km (62 miles) per hour. Once levitated, however, the train is moved forward by propulsion provided by the guideway coils, which are constantly changing polarity owing to alternating electrical current that powers the system.
Maglevs eliminate a key source of friction—that of train wheels on the rails—although they must still overcome air resistance. This lack of friction means that they can reach higher speeds than conventional trains. At present maglev technology has produced trains that can travel in excess of 500 km (310 miles) per hour. This speed is twice as fast as a conventional commuter train and comparable to the TGV (Train à Grande Vitesse) in use in France, which travels between 300 and 320 km (186 and 199 miles) per hour. Because of air resistance, however, maglevs are only slightly more energy efficient than conventional trains.
Benefits and costs
Maglevs have several other advantages compared with conventional trains. They are less expensive to operate and maintain, because the absence of rolling friction means that parts do not wear out quickly (as do, for instance, the wheels on a conventional railcar). This means that fewer materials are consumed by the train’s operation, because parts do not constantly have to be replaced. The design of the maglev cars and railway makes derailment highly unlikely, and maglev railcars can be built wider than conventional railcars, offering more options for using the interior space and making them more comfortable to ride in. Maglevs produce little to no air pollution during operation, because no fuel is being burned, and the absence of friction makes the trains very quiet (both within and outside the cars) and provides a very smooth ride for passengers. Finally, maglev systems can operate on higher ascending grades (up to 10 percent) than traditional railroads (limited to about 4 percent or less), reducing the need to excavate tunnels or level the landscape to accommodate the tracks.
The greatest obstacle to the development of maglev systems is that they require entirely new infrastructure that cannot be integrated with existing railroads and that would also compete with existing highways, railroads, and air routes. Besides the costs of construction, one factor to be considered in developing maglev rail systems is that they require the use of rare-earth elements (scandium, yttrium, and 15 lanthanides), which may be quite expensive to recover and refine. Magnets made from rare-earth elements, however, produce a stronger magnetic field than ferrite (iron compounds) or alnico (alloys of iron, aluminum, nickel, cobalt, and copper) magnets to lift and guide the train cars over a guideway.
Maglev systems
Several train systems using maglev have been developed over the years, with most operating over relatively short distances. Between 1984 and 1995 the first commercial maglev system was developed in Great Britain as a shuttle between the Birmingham airport and a nearby rail station, some 600 meters (about 1,970 feet) away. Germany constructed a maglev in Berlin (the M-Bahn) that began operation in 1991 to overcome a gap in the city’s public transportation system caused by the Berlin Wall; however, the M-Bahn was dismantled in 1992, shortly after the wall was taken down. The 1986 World’s Fair (Expo 86) in Vancouver included a short section of a maglev system within the fairgrounds.
Six commercial maglev systems are currently in operation around the world. One is located in Japan, two in South Korea, and three in China. In Aichi, Japan, near Nagoya, a system built for the 2005 World’s Fair, the Linimo, is still in operation. It is about 9 km (5.6 miles) long, with nine station stops over that distance, and reaches speeds of about 100 km (62 miles) per hour. The Korean Rotem Maglev runs in the city of Taejeŏn between the Taejeŏn Expo Park and the National Science Museum, a distance of 1 km (0.6 mile). The Inch’ŏn Airport Maglev has six stations and runs from Inch’ŏn International Airport to the Yongyu station, 6.1 km (3.8 miles) away. The longest commercial maglev system is in Shanghai; it covers about 30 km (18.6 miles) and runs from downtown Shanghai to Pudong International Airport. The line is the first high-speed commercial maglev, operating at a maximum speed of 430 km (267 miles) per hour. China also has two low-speed maglev system operating at speeds of 100 km (62 miles) per hour. The Changsha Maglev connects that city’s airport to a station 18.5 km (11.5 miles) away, and the S1 line of the Beijing subway system has seven stops over a distance of 9 km (6 miles).
Japan has plans to create a long-distance high-speed maglev system, the Chuo Shinkansen, which would connect Nagoya to Tokyo, a distance of 286 km (178 miles), with an extension to Osaka (438 km [272 miles] from Tokyo) planned for 2037. However, the project was delayed past its original deadline in 2027 when the governor of Shizuoka Prefecture opposed the geological survey necessary to accommodate the high-speed train, citing impacts on biodiversity and water supply (though many surmised that it was because Shizuoka was the one prefecture with no station on the line). The governor’s resignation in 2024 effectively resumed the project, with new estimates placing the Nagoya-Tokyo line’s completion in 2034. The Chuo Shinkansen is planned to travel at 500 km (310 miles) per hour and make the Tokyo-Osaka trip in 67 minutes.
Details
Maglev (derived from magnetic levitation) is a system of rail transport whose rolling stock is levitated by electromagnets rather than rolled on wheels, eliminating rolling resistance.
Compared to conventional railways, maglev trains have higher top speeds, superior acceleration and deceleration, lower maintenance costs, improved gradient handling, and lower noise. However, they are more expensive to build, cannot use existing infrastructure, and use more energy at high speeds.
Maglev trains have set several speed records. The train speed record of 603 km/h (375 mph) was set by the experimental Japanese L0 Series maglev in 2015. From 2002 until 2021, the record for the highest operational speed of a passenger train of 431 kilometres per hour (268 mph) was held by the Shanghai maglev train, which uses German Transrapid technology. The service connects Shanghai Pudong International Airport and the outskirts of central Pudong, Shanghai. At its historical top speed, it covered the distance of 30.5 kilometres (19 mi) in just over 8 minutes (average speed: 228.75 km/h).
Different maglev systems achieve levitation in different ways, which broadly fall into two categories: electromagnetic suspension (EMS) and electrodynamic suspension (EDS). Propulsion is typically provided by a linear motor. The power needed for levitation is typically not a large percentage of the overall energy consumption of a high-speed maglev system. Instead, overcoming drag takes the most energy. Vactrain technology has been proposed as a means to overcome this limitation.
Despite over a century of research and development, there are only seven operational maglev trains today — four in China, two in South Korea, and one in Japan.
Two inter-city maglev lines are currently under construction, the Chūō Shinkansen connecting Tokyo and Nagoya (with further connection to Osaka) and a line between Changsha and Liuyang in Hunan Province, China.
Additional Information
The evolution of mass transportation has fundamentally shifted human civilization. In the 1860s, a transcontinental railroad turned the months-long slog across America into a week-long journey. Just a few decades later, passenger automobiles made it possible to bounce across the countryside much faster than on horseback. And of course, during the World War I era, the first commercial flights began transforming our travels all over again, making coast-to-coast journeys a matter of hours. But rail trips in the U.S. aren't much faster today than they were a century ago. For engineers looking for the next big breakthrough, perhaps "magical" floating trains are just the ticket.
In the 21st century there are a few countries using powerful electromagnets to develop high-speed trains, called maglev trains. These trains float over guideways using the basic principles of magnets to replace the old steel wheel and track trains. There's no rail friction to speak of, meaning these trains can hit speeds of hundreds of miles per hour.
Yet high speed is just one major benefit of maglev trains. Because the trains rarely (if ever) touch the track, there's far less noise and vibration than typical, earth-shaking trains. Less vibration and friction results in fewer mechanical breakdowns, meaning that maglev trains are less likely to encounter weather-related delays.
The first patents for magnetic levitation (maglev) technologies were filed by French-born American engineer Emile Bachelet all the way back in the early 1910s. Even before that, in 1904, American professor and inventor Robert Goddard had written a paper outlining the idea of maglev levitation [source: Witschge]. It wasn't long before engineers began planning train systems based on this futuristic vision. Soon, they believed, passengers would board magnetically propelled cars and zip from place to place at high speed, and without many of the maintenance and safety concerns of traditional railroads.
The big difference between a maglev train and a conventional train is that maglev trains do not have an engine — at least not the kind of engine used to pull typical train cars along steel tracks. The engine for maglev trains is rather inconspicuous. Instead of using fossil fuels, the magnetic field created by the electrified coils in the guideway walls and the track combine to propel the train.
If you've ever played with magnets, you know that opposite poles attract and like poles repel each other. This is the basic principle behind electromagnetic propulsion. Electromagnets are similar to other magnets in that they attract metal objects, but the magnetic pull is temporary. You can easily create a small electromagnet yourself by connecting the ends of a copper wire to the positive and negative ends of an AA, C or D-cell battery. This creates a small magnetic field. If you disconnect either end of the wire from the battery, the magnetic field is taken away.
The magnetic field created in this wire-and-battery experiment is the simple idea behind a maglev train rail system. There are three components to this system:
* A large electrical power source
* Metal coils lining a guideway or track
* Large guidance magnets attached to the underside of the train.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2704 2026-02-23 17:21:04
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2503) South Pole
Gist
The South Pole, located at the southernmost point on Earth (90°S) in Antarctica, is an extremely cold, high-altitude (~9,300 ft elevation) desert. It has a population of roughly 50 people in winter and hundreds in summer, supported by the U.S. Amundsen-Scott Station. Key challenges include extreme, life-threatening temperatures (down to
),6 months of darkness, and absolute isolation.
Summary
The South Pole, also known as the Geographic South Pole or Terrestrial South Pole, is the point in the Southern Hemisphere where the Earth's axis of rotation meets its surface. It is called the True South Pole to distinguish from the south magnetic pole.
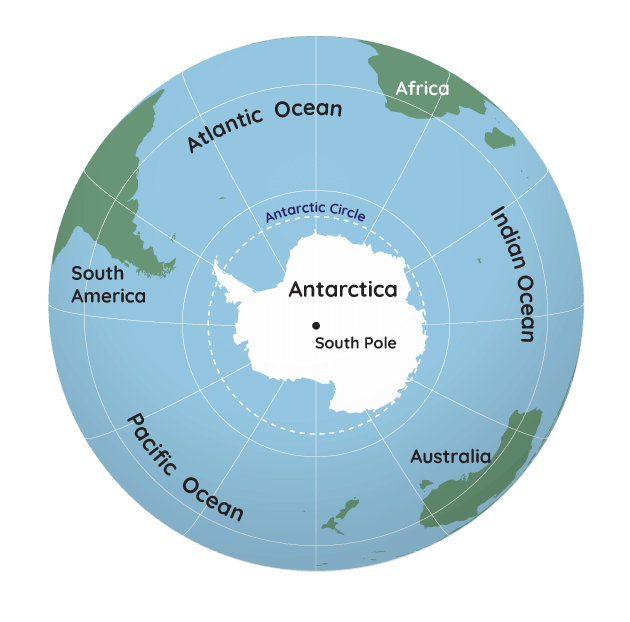
The South Pole is by definition the southernmost point on the Earth, lying antipodally to the North Pole. It defines geodetic latitude 90° South, as well as the direction of true south. At the South Pole all directions point North; all lines of longitude converge there, so its longitude can be defined as any degree value. No time zone has been assigned to the South Pole, so any time can be used as the local time. Along tight latitude circles, clockwise is east and counterclockwise is west. The South Pole is at the center of the Southern Hemisphere. Situated on the continent of Antarctica, it is the site of the United States Amundsen–Scott South Pole Station, which was established in 1956 and has been permanently staffed since that year.
Because the South Pole is covered by an ice sheet roughly 3.2 km (2.0 mi) thick that is slowly moving, the geographic marker must be moved several meters each year. Also, buildings slowly become buried in snow because it does not melt. There is a marker at the geographic South Pole placed each year, and also a Ceremonial South Pole marked with various flags and a special post.
Details
The South Pole is the southernmost point on Earth. It is the precise point of the southern intersection of Earth's axis and Earth's surface.
From the South Pole, all directions are north. Its latitude is 90 degrees south, and all lines of longitude meet there (as well as at the North Pole).
The South Pole is located on Antarctica, one of Earth's seven continents. Although land at the South Pole is only about a hundred meters above sea level, the ice sheet above it is roughly 2,700-meters (9,000-feet) thick. This elevation makes the South Pole much colder than the North Pole, which sits in the middle of the Arctic Ocean. In fact, the warmest temperature ever recorded at the South Pole was a freezing -12.3 degrees Celsius (9.9 degrees Fahrenheit).
The South Pole is close to the coldest place on Earth. The coldest temperature recorded at the South Pole, -82.8 degrees Celsius (-117.0 degrees Fahrenheit), is still warmer than the coldest temperature ever recorded, -89.2 degrees Celsius (-128.6 degrees Fahrenheit). That temperature was recorded at the Russian Vostok Research Station, about 1,300 kilometers (808 miles) away.
Because Earth rotates on a tilted axis as it revolves around the sun, sunlight is experienced in extremes at the poles. In fact, the South Pole experiences only one sunrise (at the September equinox) and one sunset (at the March equinox) every year. From the South Pole, the sun is always above the horizon in the summer and below the horizon in the winter. This means the region experiences up to 24 hours of sunlight in the summer and 24 hours of darkness in the winter.
Due to plate tectonics, the exact location of the South Pole is constantly moving. Plate tectonics is the process of large slabs of Earth's crust moving slowly around the planet, bumping into and pulling apart from one another.
Over billions of years, Earth's continents have shifted together and drifted apart. Millions of years ago, land that today is the east coast of South America was at the South Pole. Today, the ice sheet above the South Pole drifts about 10 meters (33 feet) every year.
Amundsen–Scott South Pole Station
Compared to the North Pole, the South Pole is relatively easy to travel to and study. The North Pole is in the middle of the Arctic Ocean, while the South Pole is on a stable piece of land.
The United States has had scientists working at Amundsen–Scott South Pole Station since 1956. Between 50 and 200 scientists and support staff live at the this research station at any given time. The station itself does not sit on the ground or ice sheet. It is able to adjust its elevation, to prevent it from being buried in snow, which accumulates at a rate of about 20 centimeters (eight inches) every year, and does not melt.
In the winter, the Amundsen–Scott South Pole Station is completely self-sufficient. The dark sky, freezing temperatures, and gale-force winds prevent most supplies from being flown or trekked in. All food, medical supplies, and other material must be secured before the long Antarctic winter. The station's energy is provided by three enormous generators that run on jet fuel.
In winter, stores of food are supplemented by the Amundsen–Scott South Pole Station's greenhouse. Vegetables in the greenhouse are grown with hydroponics, in a nutrient solution instead of soil.
Some of the earliest discoveries made at South Pole research stations helped support the theory of continental drift, the idea that continents drift apart and shift together. Rock samples collected near the South Pole and throughout Antarctica match samples dated to the same time period collected at tropical latitudes. Geologists conclude that the samples formed at the same time and the same place, and were torn apart over millions of years, as the planet split into different continents.
Today, the Amundsen–Scott South Pole Station is host to a wide variety of research. The relatively undisturbed ice sheet maintains a pristine record of snowfalls, air quality, and weather patterns. Ice cores provide data for glaciologists, climatologists, and meteorologists, as well as scientists tracking patterns in climate change.
The South Pole has low temperatures and humidity and high elevation, making it an outstanding place to study astronomy and astrophysics. The South Pole Telescope studies low-frequency radiation, such as microwaves and radio waves. The South Pole Telescope is one of the instruments designed measure the cosmic microwave background (CMB)–faint, diffuse radiation left over from the Big Bang.
Astrophysicists also search for tiny particles called neutrinos at the South Pole. Neutrinos interact very, very weakly with all other matter. Neutrino detectors therefore must be very large to detect a measurable number of the particles. The Amundsen–Scott South Pole Station's IceCube Neutrino Detector has more than 80 "strings" of sensors reaching as deep as 2,450 meters (8,038 feet) beneath the ice. It is the largest neutrino detector in the world.
Ecosystems at the South Pole
Although the Antarctic coast is teeming with marine life, few biologists conduct research at the Amundsen–Scott South Pole Station. The habitat is far too harsh for most organisms to survive.
In fact, the South Pole sits in the middle of the largest, coldest, driest, and windiest desert on Earth. More temperate parts of this desert (called either East Antarctica or Maudlandia) support native flora such as moss and lichen, and organisms such as mites and midges. The South Pole itself has no native plant or animal life at all. Sometimes, however, seabirds such as skuas can be spotted if they are blown off-course.
Exploration
The early 20th century's "Race to the Pole" stands as a symbol of the harrowing nature of polar exploration.
European and American explorers had attempted to reach the South Pole since British Capt. Robert Falcon Scott's expedition of 1904. Scott, along with fellow Antarctic explorers Ernest Shackleton and Edward Wilson, came within 660 kilometers (410 miles) of the pole, but turned back due to weather and inadequate supplies.
Shackleton and Scott were determined to reach the pole. Scott worked with scientists, intent on using the best techniques to gather data and collect samples.
Shackleton also conducted scientific surveys, although his expeditions were more narrowly focused on reaching the South Pole. He came within 160 kilometers (100 miles) of the pole in 1907, but again had to turn back due to weather.
Scott gathered public support and public funding for his 1910 Terra Nova expedition. He secured provisions and scientific equipment. In addition to the sailors and scientists on his team, the Terra Nova expedition also included tourists—guests who helped finance the voyage in exchange for taking part in it.
On the way to Antarctica, the Terra Nova expedition stopped in Australia to take on final supplies. Here, Scott received a surprising telegram from Norwegian explorer Roald Amundsen: "Beg leave to inform you Fram [Amundsen's ship] proceeding Antarctic."
Amundsen was apparently racing for the pole, ahead of Scott, but had kept all preparation secret. His initial ambition, to be the first to reach the North Pole, had been thwarted by American explorers Frederick Cook and Robert Peary, both of whom claimed to reach the North Pole first. (Both claims are now disputed, and Amundsen's flight over the North Pole is generally recognized as the first verified journey there.)
The Terra Nova and Fram expeditions arrived in Antarctica about the same time, in the middle of the Antarctic summer (January). They set up base camps about 640 kilometers (400 miles) apart. As they proceeded south, both expeditions established resupply depots with supplies for their return journey. While Scott's team stuck to a route forged by Shackleton years earlier, Amundsen took a new route.
Scott proceeded with scientific and expeditionary equipment hauled by dogs, ponies, and motor sledges. The motorized equipment soon broke down, and the ponies could not adapt to the harsh Antarctic climate. Even the sled dogs became weary. All the ponies died, and most members of the expedition turned back. Only four men from the Terra Nova expedition (including Scott's friend Wilson) proceeded with Scott to the pole.
Amundsen traveled by dogsled, with a team of explorers, skiers, and mushers. The foresight and navigation paid off: Amundsen reached the pole in December 1911. He called the camp Polheim, and the entire Fram expedition successfully returned to their resupply depots, ship, and Norway.
More than a month later, Scott reached the South Pole, only to be met by Amundsen's camp—he had left a tent, equipment, and supplies for Scott, as well as a note for the King of Norway to be delivered if the Fram expedition failed to make it back.
Disheartened, Scott's team slowly headed back north. They faced colder temperatures and harsher weather than Amundsen's team. They had fewer supplies. Suffering from hunger, hypothermia, and frostbite, all members of Scott's South Pole expedition died fewer than 18 kilometers (11 miles) from a resupply depot.
American explorer Richard E. Byrd became the first person to fly over the South Pole, in 1926, and the Amundsen–Scott South Pole Station was established 30 years later.
However, the next overland expedition to the South Pole was not made until 1958, more than 40 years after Amundsen and Scott's deadly race. The 1958 expedition was led by legendary New Zealand mountaineer Sir Edmund Hillary, who had become the first person to scale Mount Everest in 1953.
Transportation to the South Pole
Almost all scientists and support personnel, as well as supplies, are flown in to the South Pole. Hardy military aircraft usually fly from McMurdo Station, an American facility on the Antarctic coast and the most populated area on the continent. The extreme and unpredictable weather around the pole can often delay flights.
In 2009, the U.S. completed construction of the South Pole Traverse. Also called the McMurdo-South Pole Highway, this stretch of unpaved road runs more than 1,600 kilometers (995 miles) over the Antarctic ice sheet, from McMurdo Station to the Amundsen–Scott South Pole Station. It takes about 40 days for supplies to reach the pole from McMurdo, but the route is far more reliable and inexpensive than air flights. The highway can also supply much heavier equipment (such as that needed by the South Pole's astrophysics laboratories) than aircraft.
Resources and Territorial Claims
The entire continent of Antarctica has no official political boundaries. Seven countries made defined claims to Antarctic territory prior to the Antarctic Treaty of 1959, which does not legally recognize any claims.
Additional Information
The pole is situated about 1,300km (800 miles) inland from the nearest open sea, it is at an altitude of 2,835m (9,300ft) above sea level due to the enormous thickness of the Antarctic ice sheet. The bedrock at the pole is thought to actually be about 57m (187ft) below sea level, in part due to the weight of all that ice pushing it down.
At the surface at the South Pole, there is just snow and ice, there are no other natural significant features, no mountains sticking through the ice (there are hills and mountains beneath the ice, but they aren't tall enough to reach through) no rock, no solid ground, just a vast endless plateau of more snow and more ice.
Oh yes, and a huge human settlement that is the Amundsen-Scott South Pole Station. This American run scientific station was established in 1956 and has been permanently manned ever since then. The current station is the third to be built, work started on it in 2003. In addition to the main station building there is a large collection of other structures in the area. Some are specifically designed and constructed scientific buildings, others are sturdy insulated tents that are used for temporary summer-only accommodation. There are cabooses or converted shipping containers that are fitted out for a particular purpose or scientific experiment.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2705 2026-02-25 00:48:00
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2504) Hydraulic Press
Gist
A hydraulic press works on the principle of Pascal's law, which states that when pressure is applied to a confined fluid, the pressure change occurs throughout the entire fluid.
In hydraulic presses, Pascal's law is applied: pressure in a confined fluid is transmitted equally in all directions. In mechanical presses, kinetic energy is stored in a flywheel and transmitted via clutch/crank mechanisms to the ram.
Summary
A hydraulic press uses a hydraulic cylinder to produce a compressive force. Within a hydraulic press, there is a plate where the sample is placed to be pressed for sample preparation.
How Does a Hydraulic Press Work?
A hydraulic press works on the principle of Pascal’s law, which states that when pressure is applied to a confined fluid, the pressure change occurs throughout the entire fluid. Within the hydraulic press, there is a piston that works as a pump, that provides a modest mechanical force to a small area of the sample. There is also a piston with a larger area, which produces a larger mechanical force.
Advantages
There are a variety of advantages to using hydraulic presses. This is evident in hand-fed hydraulic systems, where the ease and speed of sample switching is considerably improved.
These instruments are also extremely beneficial for high-volume sample preparation, also increasing the speed of sampling.
Details
A hydraulic press is a machine press using a hydraulic cylinder to generate a compressive force. It uses the hydraulic equivalent of a mechanical lever, and was also known as a Bramah press after the inventor, Joseph Bramah. He invented and was issued a patent on this press in 1795. As Bramah installed toilets and developed the modern flush toilet, he studied existing literature on the motion of fluids to develop the press.
Main principle
The hydraulic press depends on Pascal's principle. The pressure throughout a closed system is constant. One part of the system is a piston acting as a pump, with a modest mechanical force acting on a small cross-sectional area; the other part is a piston with a larger area which generates a correspondingly large mechanical force. Only small-diameter tubing (which more easily resists pressure) is needed if the pump is separated from the press cylinder.
Application
Hydraulic presses are commonly used for assembly and disassembly of tightly-fitting components. In manufacturing, they are used for forging, clinching, molding, blanking, punching, deep drawing, and metal forming operations. Hydraulic presses are also used for stretch forming, rubber pad forming, and powder compacting. The hydraulic press is advantageous in manufacturing, as it gives the ability to create more intricate shapes than other methods and can be economical with materials. A hydraulic press will take up less space compared to a mechanical press of the same capability. Hydraulic presses are also used for waste processing operations such as in garbage trucks and car crushers to reduce the size of waste material for easier more economic transportation.
In geology a tungsten carbide coated hydraulic press is used in the rock crushing stage of preparing samples for geochemical analyses in topics such as understanding the origins of volcanism.
In popular culture
The room featured in Fermat's Room has a design similar to that of a hydraulic press. Boris Artzybasheff also created a drawing of a hydraulic press, in which the press was created out of the shape of a robot.
In 2015, the Hydraulic Press Channel, a YouTube channel dedicated to crushing objects with a hydraulic press, was created by Lauri Vuohensilta, a factory owner from Tampere, Finland. The Hydraulic Press Channel has since grown to over 10 million subscribers on YouTube. There are numerous other YouTube channels that publish videos involving hydraulic presses that are tasked with crushing many different items, such as bowling balls, soda cans, plastic toys, and metal tools.
A hydraulic press is featured prominently in the Sherlock Holmes story "The Adventure of the Engineer's Thumb".
Additional Information
A hydraulic press, by definition, is a mechanical apparatus that leverages the static pressure of a liquid as explained by Pascal's principle. It's employed to form, reshape, and alter various materials including metals, plastics, rubber, and wood. The primary components of a hydraulic press comprise the mainframe, the power system, and the control mechanisms.
According to Pascal's principle, if pressure is exerted on a confined fluid, the pressure change spreads consistently throughout the liquid. In a hydraulic press, this applied pressure emanates from a piston, acting similarly to a pump to produce mechanical force.
The hydraulic press is a powerful machine widely used in industrial applications for metal forming, assembly, molding, and material compaction. The hydraulic press operates by forcing hydraulic fluid into a double-acting piston, relying on Pascal's Law to multiply force for heavy-duty tasks. The compressive force generated within the smaller hydraulic cylinder pushes the hydraulic oil (fluid) into a larger cylinder, where much greater force and pressure are applied. As the larger piston moves, it forces the fluid back into the smaller piston cylinder, maintaining a constant hydraulic pressure throughout the system.
This controlled fluid exchange between the two pistons increases mechanical pressure, creating the substantial force needed to drive the anvil of the hydraulic press downward onto a workpiece, shaping, compacting, or cutting the material into its desired form. Once the forming, punching, or pressing process is complete, the pressure is safely released, allowing the anvil and die to return to their original positions. Hydraulic presses are highly valued for their precision, repeatability, and ability to perform a variety of material processing operations, making them a cornerstone in manufacturing, automotive, aerospace, and fabrication industries.
How a Hydraulic Press Works
A typical hydraulic press consists of two cylinders, two pipes, and two pistons. One cylinder functions as the ram, while the other acts as the plunger; they are connected by a high-strength chamber filled with hydraulic fluid, often a specialized oil designed for high-pressure environments. The configuration of these components directly enables the powerful compression and shaping abilities for which hydraulic presses are known.
* Main Cylinder (Ram): Delivers force to the workpiece.
* Plunger: Initiates pressure transfer by pushing hydraulic fluid.
* Pipes and Hoses: Ensure secure fluid movement between components, preventing leaks and ensuring safety.
* Hydraulic Fluid Reservoir: Stores and supplies fluid to support continuous operation.
* Control Valves: Direct fluid flow, manage pressure, and ensure precise operation for various press functions such as forging, stamping, and embossing.
Ram
In advanced hydraulic systems, multiple rams are used, and the number depends on the required working load. Utilizing several smaller rams rather than a single larger one allows for finer control over the hydraulic thrust force, which is essential for delicate metal forming or precision stamping. Hydraulic fluid is routed to these rams by a hydraulic pump and an accumulator, which moderates pressure between the rams and pump, ensuring optimal performance for high-tonnage applications such as deep drawing, blanking, or coining.
Accumulator
The hydraulic accumulator is a critical component that stores pressurized hydraulic fluid, releasing it as needed to maintain system efficiency and responsiveness. It typically consists of a durable cylinder with a spring-loaded or pneumatic piston separator. The accumulator functions as an energy storage device, enabling the hydraulic press to quickly respond to sudden demands without requiring the hydraulic pump to operate continuously. The constant pressure provided by the accumulator is crucial for consistent operation in heavy manufacturing processes, energy efficiency, and reducing mechanical wear. Properly sized accumulators enhance the safety, speed, and reliability of industrial hydraulic press systems.
Pump
There are three main types of hydraulic pumps used in presses: vane, gear, and piston, with piston pumps prevailing in high-performance equipment due to their efficiency and durability under high loads. Hydraulic presses utilize positive displacement pumps, which deliver a precise, constant volume of hydraulic oil during each cycle, maintaining high forces required in automotive component manufacturing, metal stamping, and plastic molding applications. Positive displacement pumps can be either fixed or variable; fixed pumps operate at set speeds, while variable pumps allow for speed and direction changes, enabling customized pressure control based on specific pressing or forming requirements. Piston pumps—available as axial, bent axis, or radial designs—are especially suited for hydraulic press systems because they handle high pressure, provide superior volumetric efficiency, and minimize fluid leakage, ensuring long-term operational reliability in industrial and commercial environments.
Cylinders
The number and size of cylinders in a hydraulic press depend on the design and intended tonnage capacity. These cylinders generate the immense compressive force that drives the press ram and die to shape or cut metal, plastic, rubber, or composites. In a typical two-cylinder design, the cylinder paired with the ram has a larger diameter to produce maximum force, while the plunger cylinder is smaller and initiates fluid movement. Both are made from robust, pressure-rated steel, featuring input/output ports for controlled hydraulic fluid circulation to support heavy pressing operations.
Cylinders are interconnected via hydraulic pipes and hoses, which transmit high-pressure fluid. When the plunger's downward stroke applies pressure to the hydraulic oil, the resulting force is transferred to the main ram. This unidirectional force—delivered via a linear actuator—enables consistent, dynamic motion, critical for applications such as metalforming, compression molding, powder compacting, and precision stamping.
Hydraulic Press Process
The hydraulic press process is the foundation of modern metal forming, fabrication, and materials engineering. The animation below demonstrates how consistent hydraulic pressure from the system's cylinders powers the main ram, driving the press anvil downward onto the workpiece or slug positioned in the die cavity. The result is precise, repeatable compression, shaping, or assembly of materials into components for the automotive, aerospace, electronics, and appliance industries. Because hydraulic presses can deliver adjustable force, stroke length, and speed, they are ideal for a diverse range of processes, including forging, deep drawing, extrusion, lamination, and powder metallurgy. Their versatility and controllability ensure ideal results and cost-effective production in both high-volume and custom-manufacturing environments.
Choosing the Right Hydraulic Press for your production needs involves evaluating not only the type of hydraulic system, but also key factors such as required tonnage, workspace dimensions, safety features, energy consumption, and cycle speed. Leading hydraulic press manufacturers offer custom solutions designed for processes such as metal stamping, plastic injection, rubber molding, and powder compaction. When evaluating suppliers and comparing models, consider the quality of components (cylinders, pumps, seals, frames), after-sales technical support, and maintenance requirements to ensure long-term reliability and maximum return on investment.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2706 2026-02-26 00:55:40
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2505) Atrophy
Gist
Atrophy is the wasting away, thinning, or decrease in size of cells, tissues, or organs, resulting in reduced function. It is caused by factors like disuse, poor circulation, nerve damage, malnutrition, or hormonal changes. Common forms include muscle, brain, or vaginal atrophy, often characterized by weakness and reduced size of the affected area.
Brain atrophy means the progressive loss of brain cells (neurons) and their connections, causing the brain to shrink in overall size or in specific regions, leading to impaired cognitive, motor, or functional abilities, and can be a normal part of aging or a symptom of diseases like Alzheimer's or MS (Multiple Sclerosis). It's diagnosed via brain scans like MRIs and CTs, which reveal the tissue loss, and treatment focuses on managing the underlying cause.
Summary
Muscle atrophy is the wasting or thinning of muscle mass. It can be caused by disuse of your muscles or neurogenic conditions. Symptoms include a decrease in muscle mass, one limb being smaller than the other, and numbness, weakness and tingling in your limbs. Disuse atrophy can be reversed with exercise and a healthy diet.
Muscle atrophy is the loss or thinning of your muscle tissue. If you have atrophied muscles, you’ll see a decrease in your muscle mass and strength. With muscle atrophy, your muscles look smaller than normal. Muscle atrophy can occur due to malnutrition, age, genetics, a lack of physical activity or certain medical conditions. Disuse (physiologic) atrophy occurs when you don’t use your muscles enough. Neurogenic atrophy occurs due to nerve problems or diseases.
What are the symptoms of muscle atrophy?
The symptoms of muscle atrophy differ depending on the cause of your condition. The most obvious sign of muscle atrophy is reduced muscle mass. Other signs of muscle atrophy may include:
* One arm or one leg is smaller than the other.
* Weakness in one arm and or one leg.
* Numbness or tingling in your arms and legs.
* Trouble walking or balancing.
* Difficulty swallowing or speaking.
* Facial weakness.
* Gradual memory loss.
Details
Atrophy is the partial or complete wasting away of a part of the body. Causes of atrophy include mutations (which can destroy the gene to build up the organ), poor nourishment, poor circulation, loss of hormonal support, loss of nerve supply to the target organ, excessive amount of apoptosis of cells, and disuse or lack of exercise or disease intrinsic to the tissue itself. In medical practice, hormonal and nerve inputs that maintain an organ or body part are said to have trophic effects. A diminished muscular trophic condition is designated as atrophy. Atrophy is reduction in size of cell, organ or tissue, after attaining its normal mature growth. In contrast, hypoplasia is the reduction in the cellular numbers of an organ, or tissue that has not attained normal maturity.
Atrophy is the general physiological process of reabsorption and breakdown of tissues, involving apoptosis. When it occurs as a result of disease or loss of trophic support because of other diseases, it is termed pathological atrophy, although it can be a part of normal body development and homeostasis as well.
Examples of atrophy as part of normal development include shrinking and the involution of the thymus in early childhood, and the tonsils in adolescence. In old age, effects include, but are not limited to, loss of teeth, hair, thinning of skin that creates wrinkles, weakening of muscles, loss of weight in organs and sluggish mental activity.
Muscle atrophies
Disuse atrophy of muscles and bones, with loss of mass and strength, can occur after prolonged immobility, such as extended bedrest, or having a body part in a cast (living in darkness for the eye, bedridden for the legs etc.). This type of atrophy can usually be reversed with exercise unless severe.
There are many diseases and conditions which cause atrophy of muscle mass. For example, diseases such as cancer and AIDS induce a body wasting syndrome called cachexia, which is notable for the severe muscle atrophy seen. Other syndromes or conditions which can induce skeletal muscle atrophy are congestive heart failure and liver disease.
During aging, there is a gradual decrease in the ability to maintain skeletal muscle function and mass. This condition is called sarcopenia, and may be distinct from atrophy in its pathophysiology. While the exact cause of sarcopenia is unknown, it may be induced by a combination of a gradual failure in the satellite cells which help to regenerate skeletal muscle fibers, and a decrease in sensitivity to or the availability of critical secreted growth factors which are necessary to maintain muscle mass and satellite cell survival.
Dystrophies, myositis, and motor neuron conditions
Pathologic atrophy of muscles can occur with diseases of the motor nerves or diseases of the muscle tissue itself. Examples of atrophying nerve diseases include Charcot-Marie-Tooth disease, poliomyelitis, amyotrophic lateral sclerosis (ALS or Lou Gehrig's disease), and Guillain–Barré syndrome. Examples of atrophying muscle diseases include muscular dystrophy, myotonia congenita, and myotonic dystrophy.
Changes in Na+ channel isoform expression and spontaneous activity in muscle called fibrillation can also result in muscle atrophy.
A flail limb is a medical term which refers to an extremity in which the primary nerve has been severed, resulting in complete lack of mobility and sensation. The muscles soon wither away from atrophy.
Gland atrophy
The adrenal glands atrophy during prolonged use of exogenous glucocorticoids like prednisone. Atrophy of the breasts can occur with prolonged estrogen reduction, as with anorexia nervosa or menopause. Testicular atrophy can occur with prolonged use of enough exogenous sex steroids (either androgen or estrogen) to reduce gonadotropin secretion.
Vaginal atrophy
In post-menopausal women, the walls of the math become thinner (atrophic vaginitis). The mechanism for the age-related condition is not yet clear, though there are theories that the effect is caused by decreases in estrogen levels. This atrophy, occurring concurrently with breast atrophy, is consistent with the homeostatic (normal development) role of atrophy in general, as after menopause the body has no further functional biological need to maintain the reproductive system which it has permanently shut down.
Research
One drug in test seemed to prevent the type of muscle loss that occurs in immobile, bedridden patients. Testing on mice showed that it blocked the activity of a protein present in the muscle that is involved in muscle atrophy. However, the drug's long-term effect on the heart precludes its routine use in humans, and other drugs are being sought.
Additional Information
Atrophy is a decrease in size of a body part, cell, organ, or other tissue. The term implies that the atrophied part was of a size normal for the individual, considering age and circumstance, prior to the diminution. In atrophy of an organ or body part, there may be a reduction in the number or in the size of the component cells, or in both.
Certain cells and organs normally undergo atrophy at certain ages or under certain physiologic circumstances. In the human embryo, for example, a number of structures are transient and at birth have already undergone atrophy. The adrenal glands become smaller shortly after birth because an inner layer of the cortex has shrunk. The thymus and other lymphoid tissues atrophy at adolescence. The pineal gland tends to atrophy about the time of puberty; usually calcium deposits, or concretions, form in the atrophic tissue. The widespread atrophy of many tissues that accompanies advanced age, although universal, is influenced by changes of nutrition and blood supply that occur during active mature life.
The normal cyclic changes of female reproductive organs are accompanied by physiologic atrophy of portions of these organs. During the menstrual cycle, the corpus luteum of the ovary atrophies if pregnancy has not occurred. The muscles of the uterus, which enlarge during pregnancy, rapidly atrophy after the delivery of the child, and after completion of lactation the milk-producing acinar structures of the breast diminish in size. After menopause the ovaries, uterus, and breasts normally undergo a degree of atrophic change.
Whole body atrophy
Atrophy in general is related to changes in nutrition and metabolic activity of cells and tissues. A widespread or generalized atrophy of body tissues occurs under conditions of starvation, whether because food is unavailable or because it cannot be taken and absorbed because of the presence of disease. The unavailability of certain essential protein components and vitamins disturbs the metabolic processes and leads to atrophy of cells and tissues. Under conditions of protein starvation, the body protein is broken down into constituent amino acids, which serve to provide energy and help maintain the structure and cells of the most essential organs. The brain, heart, adrenal glands, thyroid gland, pituitary gland, gonads, and kidneys show less atrophy, relatively, than the body as a whole, whereas the fatty stores of the body, liver, spleen, and lymphoid tissues diminish relatively more than the body as a whole. The brain, heart, and kidneys, organs with abundant blood supply, appear to be the least subject to the wasting effects of starvation.
Associated with the widespread atrophy due to lack of protein is the atrophy of certain tissues that is caused by deficiencies of specific vitamins. Atrophic changes of the skin increase because of the lack of vitamin A, and atrophy of muscle increases because of the unavailability of vitamin E.
After a growth period of human metabolism, there sets in a gradual decline: slow structural changes other than those due to preventable diseases or accidents occur. Aging eventually is characterized by marked atrophy of many tissues and organs, with both a decline in the number of cells and an alteration in their constitution. This is reflected eventually in the changed, diminished, or lost function characteristic of old age and eventuates in death. The changes in senescence are affected by both inherited constitution and environmental influences, including disease and accident.
Atrophic changes of aging affect almost all tissues and organs, but some changes are more obvious and important. Arteriosclerosis—the thickening and hardening of arterial walls—decreases the vascular supply and usually accentuates aging processes.
Atrophy in old age is especially noticeable in the skin, characteristically flat, glossy or satiny, and wrinkled. The atrophy is caused by aging changes in the fibres of the true skin, or dermis, and in the cells and sweat glands of the outer skin. Wasting of muscle accompanied by some loss of muscular strength and agility is common in the aged. In a somewhat irregular pattern, there is shrinkage of many individual muscle fibres as well as a decrease in their number. Other changes have been observed within the muscle cells.
Increase of the pigment lipofuscin is also characteristic in the muscle fibres of the heart in the aged in a condition known as brown atrophy of the heart. Wasting of the heart muscle in old age may be accompanied by increase of fibrous and fatty tissue in the walls of the right side of the heart and by increased replacement of elastic tissue with fibrous tissue in the lining and walls of coronary arteries within the heart muscle. Abnormal deposits of the protein substance amyloid also occur with greater frequency in the atrophic heart muscle in old age.
Atrophy of the liver in the aged is also accompanied by increased lipochrome pigment in the atrophied cells.
The bones become progressively lighter and more porous with aging, a process known as osteoporosis. The reduction of bone tissue is most marked in cancellous bone—the open-textured tissue in the ends of the long bones—and in the inner parts of the cortex of these bones. In addition to changes in and loss of osteocytes, or bone cells, there is decreasing mineralization, or calcium deposit, with enhanced fragility of the bones.
Atrophy of the brain in old age is shown by narrowing of the ridges, or gyri, on the surface of the brain and by increased fluid in the space beneath the arachnoid membrane, the middle layer of the brain covering. There is shrinkage of individual neurons, with an increase in their lipochrome pigment content, as well as a decrease in their number. Sometimes the nerve fibrils have degenerated, and deposits called senile plaques may be found between the neurons, particularly in the frontal cortex and hippocampus (a ridge in the wall of an extension, or horn, of the lateral ventricle, or cavity, of the brain). Similar atrophic changes are seen in the brain in Alzheimer disease, a condition of unknown cause most likely to occur in older patients. The mental deterioration (senile dementia) of the aged is the clinical manifestation of these changes. Senile atrophy may be increased and complicated by the presence of arteriosclerosis.
Simmonds disease is a chronic deficiency of function of the pituitary gland, a form of hypopituitarism, that leads to atrophy of many of the viscera, including the heart, liver, spleen, kidneys, thyroid, adrenals, and gonads. The disease results in emaciation and death if left untreated.
A destructive or atrophic lesion affecting the pituitary gland with loss of hormones leads to atrophy of the thyroid gland, adrenal glands, and gonads and in turn brings atrophic changes to their target organs and the viscera. The decrease in size of the endocrine glands may be extreme.
Atrophy of muscle or of muscle and bone
Local atrophy of muscle, bone, or other tissues results from disuse or diminished activity or function. Although the exact mechanisms are not completely understood, decreased blood supply and diminished nutrition occur in inactive tissues. Disuse of muscle resulting from loss of motor nerve supply to the muscle (e.g., as a result of polio) leads to extreme inactivity and corresponding atrophy. Muscles become limp and paralyzed if there is destruction of the nerve cells in the spinal cord that normally activate them. The shrinkage of the paralyzed muscle fibres becomes evident within a few weeks. After some months, fragmentation and disappearance of the muscle fibres occurs with some replacement by fat cells and a loose network of connective tissue. Some contracture may result.
The skeletal muscles forced to inactivity by paralysis (e.g., of a limb as a result of polio) also undergo disuse atrophy. If there is a tendency for bone to become lighter and more porous in some particular area, a condition known as local osteoporosis, this can be recognized by X-rays within a few weeks. The cortex of the long bones becomes considerably thinned or atrophic, with decreased mineral content. Disuse as a result of painfully diseased joints, as in rheumatoid arthritis, results in a similar but lesser degree of atrophy of muscles concerned with movement of the involved joint, and local atrophy may also occur in the bone in the neighbourhood of the joint. A local osteoporosis of bone known as Sudeck atrophy sometimes develops rapidly in the area of an injury to bone.
Severe or prolonged deficits of blood sugar deprive the nervous system of needed sources of energy and as a rare event result in degeneration of cells of the brain and peripheral nerves. The disuse atrophy of muscle or bone that may result is fundamentally similar to the other disuse atrophies of these tissues.
Persistent pressure will cause atrophy of a compressed cell, organ, or tissue, presumably because of interference with the nutrition and metabolic activity of the affected part. Cells in a local area (e.g., in the liver) atrophy from the pressure of materials such as amyloid deposited around them. The pressure of an expanding benign tumour causes atrophy of adjacent normal structures. The pressure of a localized dilatation of an artery (aneurysm) will cause atrophy of tissues, even bone, on which it impinges.
Bulging of an intervertebral disk or growth of a tumour sometimes brings pressure on nerves near their point of exit from the spinal cord; if the pressure is prolonged, the muscles normally controlled by these nerves may atrophy. Most often the calf muscles are affected. Pressure as a result of involvement of the vertebrae at the level of the neck, or from compression of the network of nerves called the brachial plexus by the scalenus anticus muscle, produces similar effects in the upper chest and arms.
Simple disuse of muscle or bone, as, for example, from the immobilization produced when a limb is put in a cast or sling, results in atrophy of these tissues. In the case of muscle, the degree of atrophy is generally less severe than that caused by injury to a nerve, although the nature of the change is similar.
Localized atrophies of leg and arm muscles may result from hereditary or familial diseases in which the nerves of the spinal cord that supply them are inactivated or destroyed. In Charcot-Marie-Tooth disease, the atrophy involves mainly the peroneal muscles, at the outer side of the lower legs, and sometimes the muscles of the hand as well. It commonly begins in childhood or adolescence. Peroneal muscle atrophy is also seen in the hereditary spinal cord degenerative disease known as Friedreich ataxia.
Atrophy of nerve tissue
Atrophy of brain or spinal cord tissue may be brought about by injuries that directly affect a localized area or that interfere with the blood supply to an area. When peripheral nerves are severed, degenerative and eventually atrophic changes ensue in the part beyond the injury. This type of atrophy is known as Wallerian degeneration. If conditions do not allow regeneration of nerve fibres from the proximal fragment of the cut nerve, atrophy is the eventual fate of the nerve tissue distal to the injury. Retrograde atrophy also occurs from disuse and affects the ganglion cells of the injured nerve.
Prolonged pressure brings about atrophy in the central nervous system as elsewhere. The pressure of an expanding tumour of the membranes covering the brain results in localized atrophy of the adjacent brain substance on which it impinges. In hydrocephalus more widespread atrophy of brain tissue results from the abnormal amounts of fluid confined within the rigid bony compartment of the skull. Increased pressure within the skull may force a portion of the brain through the foramen magnum, the bony opening at the base of the skull, and, if prolonged, results in a localized atrophy of cerebellar tissue pressed against the bony wall.
The late stages of chronic infections may be characterized by atrophy of the brain. A striking example of this is the variety of syphilitic infection of the nervous system known as general paresis in which the brain is shrunk and reduced in weight, the atrophy affecting mainly the cortex of the brain, particularly or most markedly in the frontal area. Occasionally the atrophy is local or affects only one side of the brain. The shrinkage of the brain tissue is mainly due to loss of many nerve cells of the cortex.
Atrophy of fatty tissue
Atrophy of adipose tissue of the body occurs as a part of the generalized atrophy of prolonged undernutrition. Localized atrophy of adipose tissue—lipodystrophy—may be the result of injury to the local area; e.g., repeated insulin injections cause atrophy of fatty tissue at the site of the injections. Progressive lipodystrophy is a disease of unknown cause in which the fatty tissue atrophies only in certain regions of the body. It occurs mainly in women and often begins in childhood. The progressive wasting of adipose tissue affects mainly the face, arms, and trunk. In the affected areas, the specialized fat-holding cells of adipose tissue disappear.
Atrophy of skin
A widespread atrophic change in the skin has been noted as a prominent part of the aging process. Similar atrophic changes in the skin appear to be brought about or enhanced by excessive exposure to sunlight. While a number of abnormal conditions of the skin may include localized atrophic changes in the epidermis or dermis as a part of their lesions, certain generalized diseases of the skin are particularly characterized by such changes. The hardening of the skin known as scleroderma may occur in a localized, or circumscribed, form called morphea or as a more diffuse and severe disease. Advanced stages of scleroderma are characterized by marked atrophy of the tissue and appendages of the true skin. Atrophic thinning of the overlying epidermis also may occur, and the underlying fatty tissue and muscle may atrophy as well. The chronic form of the disease discoid lupus erythematosus also is characterized by atrophy. In advanced stages atrophy occurs particularly in the epidermis in focal areas. The thinned layer of epidermis may be a prominent feature of the microscopic appearance of the skin.
Atrophy of glands
Endocrine glandular tissues may undergo atrophy when an excess of their hormonal product is present as a result of disease. An example is seen in connection with a hormone-producing tumour of the cortical tissue of one adrenal gland, which may be accompanied by marked atrophy of the cortical tissue of the opposite adrenal gland. This probably results from disturbance of the delicate mechanism of hormonal stimulation via the pituitary gland.
Various endocrine organs (thyroid gland, adrenal glands, gonads) depend for their activity on endocrine stimulation by hormones of the pituitary gland. A severe general failure of production of the pituitary hormones results in the widespread endocrine atrophy of Simmonds disease, as has been noted. Lesser degrees of pituitary functional disturbance may disturb a delicate balance, involving mainly one type of stimulating hormone of the pituitary, and may result in selective atrophy of the adrenal cortical tissue or of the gonads.
Glands that release their secretions through a duct (e.g., salivary glands, pancreas) may become atrophic as a result of obstruction of the duct. In the pancreas, a complete obstruction of its duct results in atrophy of the glandular tissue, except for the insulin-producing islets of Langerhans, the secretion of which is absorbed into the bloodstream. Factors of both disuse and increased pressure may be present in the atrophy resulting from obstruction of the outlet channel. Similarly, rapid and complete obstruction of a ureter is followed by atrophy of the corresponding kidney.
Chemical-induced atrophy
Cases of atrophy resulting from chemical injury are not common. In chronic math poisoning, however, degenerative changes occur in peripheral nerves, resulting in weakness and atrophy in the tissues (usually legs or arms) to which the nerves are distributed. Similar results may follow the peripheral neuropathy of chronic lead poisoning.
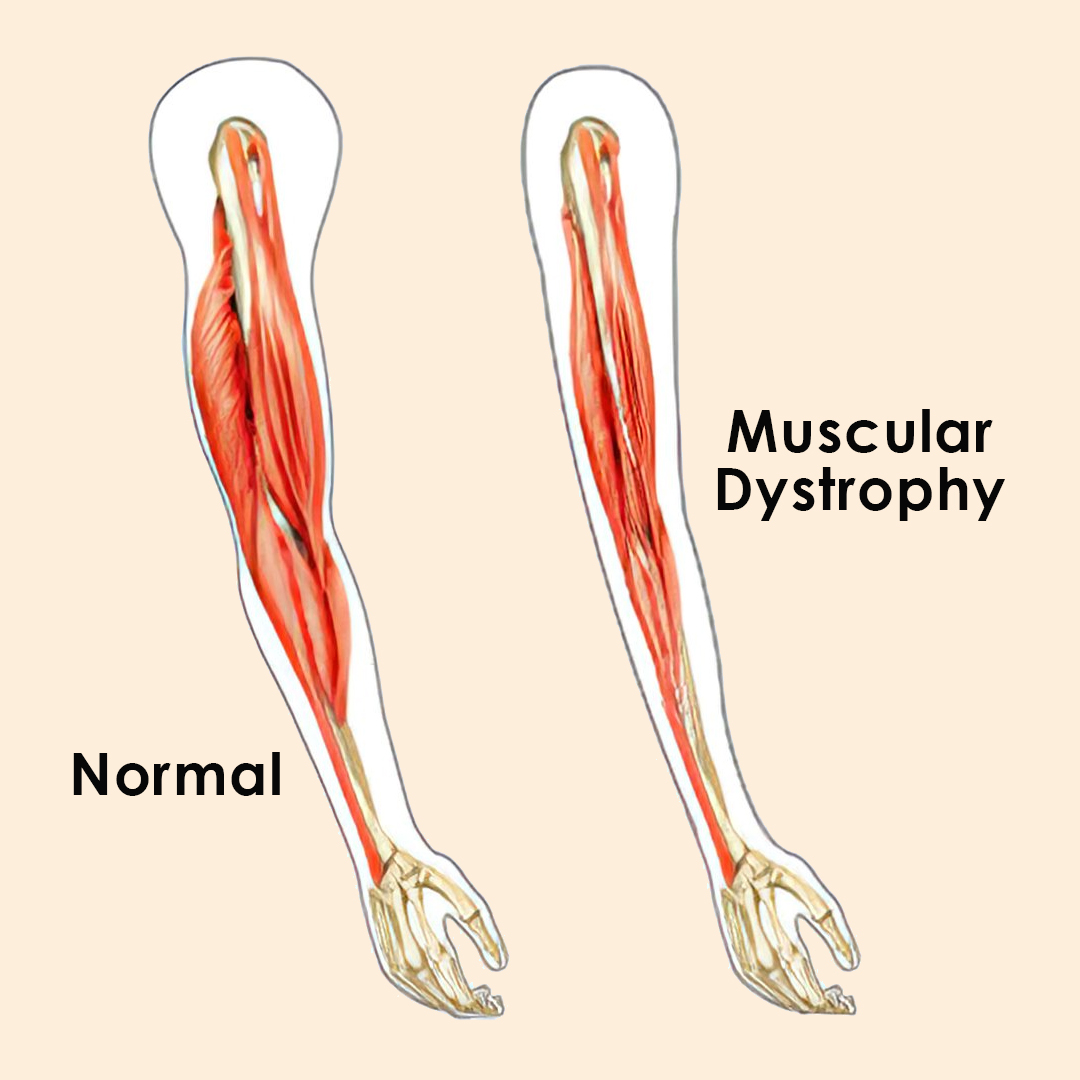
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2707 2026-02-27 00:02:44
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2506) Mountain Lion
Mountain Lion
Gist
Mountain lions are known by many names, including cougar, puma, catamount, painter, panther, and many more. They are the most wide-ranging cat species in the world and are found as far north as Canada and as far south as Chile.
The puma (Puma concolor) is a large cat belonging to the felidae family. It is similar in size to the jaguar, and is found is a wide variety of habitats throughout the Americas. It is also known as the cougar, mountain lion and a number of other names.
Summary
The cougar (Puma concolor), also called puma, mountain lion, catamount, and panther, is a large small cat native to the Americas. It inhabits North, Central and South America, making it the most widely distributed wild, terrestrial mammal in the Western Hemisphere, and one of the most widespread in the world. Its range spans Yukon, British Columbia and Alberta in Canada, the Rocky Mountains and areas in the western United States. Further south, its range extends through Mexico to the Amazon rainforest and the southern Andes Mountains in Patagonia. It is an adaptable generalist species, occurring in most American habitat types. It prefers habitats with dense underbrush and rocky areas for stalking but also lives in open areas.
The cougar is largely solitary. Its activity pattern varies from diurnality and cathemerality to crepuscularity and nocturnality between protected and non-protected areas, and is apparently correlated with the presence of other predators, prey species, livestock and humans. It is an ambush predator that pursues a wide variety of prey. Ungulates, particularly deer, are its primary prey, but it also hunts rodents. It is territorial and lives at low population densities. Individual home ranges depend on terrain, vegetation and abundance of prey. While large, it is not always the dominant apex predator in its range, yielding prey to other predators. It is reclusive and mostly avoids people. Fatal attacks on humans are rare but increased in North America as more people entered cougar habitat and built farms.
The cougar is listed as Least Concern on the IUCN Red List. Intensive hunting following European colonization of the Americas and ongoing human development into cougar habitat has caused populations to decline in most parts of its historical range. In particular, the eastern cougar population is considered to be mostly locally extinct in eastern North America since the early 20th century, with the exception of the isolated Florida panther subpopulation.
Details
The cougar is a cat of many names: Puma, mountain lion, and catamount, among others.
This adaptable predator has the widest range of any land mammal in the Western Hemisphere, and can be found in many habitats throughout the Americas, from Florida swamps to Canadian forests. In some areas, such as heavily urbanized southern California, cougars are increasingly sharing space with people.
Cougars are the world’s fourth largest wildcat after lions, tigers, and jaguars. They are stocky with large hind legs and a long tail—about a third of their length—which provides balance. Their strong back legs enable them to leap around 40 feet horizontally, or 18 feet vertically in a single jump.
Their scientific name—Puma concolor, which means “of one color” in Latin—refers to their evenly colored coat: usually a solid orange, yellow, tan, rusty brown, or gray with a white belly. In rare cases, cougars can be white, but no cases of black, or melanistic, cougars have ever been documented.
Hunting habits
Cougars hunt at dawn and dusk. They usually prey on deer, although these opportunistic predators also eat coyotes, moose, wild sheep, birds, and rodents. They even kill feral donkeys, an invasive species in California’s Death Valley National Park.
The cats silently stalk their prey, then pounce and kill them with a fatal bite to the back of the head or neck. When dealing with a large carcass, a cougar will eat as much as it can before hiding the rest to come back to later.
Harmful encounters with people are rare: Between 1924 and 2018, 74 cougar attacks—including 11 fatalities—were documented in 10 U.S. states.
Reproduction
Male cougars maintain large territories that overlap with several smaller territories of their mates. About three months after mating, a female gives birth to three or four kittens in a secluded den, where she stays for 10 days. Babies are born with camouflaged, spotted coats that fade into a solid color as they grow.
After six weeks, the family will leave the den, and kittens learn to hunt from their mother. Cougars are ready to set out on their own at around 18 months old. Males often strike out farther from their mother to avoid the threats of a rival male; one was recorded traveling 1,800 miles in search of a new home.
Hollywood cougar
Arguably the world’s most famous cougar was an animal called P-22, whose father was P-001—the first puma to be collared by the National Park Service. Born in the Santa Monica Mountains, P-22 left his birthplace to find his own territory and crossed some of the world’s busiest freeways to reach L.A.’s Griffith Park, part of the Hollywood Hills, where he lived for 10 years.
P-22 was compassionately euthanized in December 2022 when he was caught for an evaluation, which showed he was underweight, had organ failure, and was likely hit by a car.
Threats to survival
Cougars once roamed nearly all of the United States, but by the early 1900s, they were mostly hunted to extinction in the Midwest and eastern U.S. The Florida panther—a subspecies only found in Florida—survived, though today fewer than 200 individuals remain in the wild.
Overall, cougar populations are stable, and the International Union for the Conservation of Nature's Red List categorizes them as a species of least concern.
Yet throughout their wide range, the felines are threatened by poisonings from various substances, vehicle collisions, retaliatory killings, and hunting. (Learn more about cougars, also called ghost cats.)
Habitat fragmentation is also a pressing problem. Unlike P-22, most cougars can’t cross sprawling freeways, and this lack of connectivity causes low genetic diversity and inbreeding.
That’s why, in southern California, the Wallis Annenberg Wildlife Crossing will help various wildlife species safely cross U.S. Highway 101.
Additional Information
What's in a name? Mountain lion, puma, cougar, panther—these cats are known by more names than just about any other mammal! But no matter what you call them, they're still the same cat, Puma concolor, the largest of the "small cats." So why do we call them so many different names? Mostly because they have such a large range, and people from different countries have called them different things.
Early Spanish explorers of North and South America called them leon (lion) and gato monte (cat of the mountain), from which we get the name "mountain lion." “Puma” is the name the Incas gave these cats in their language. “Cougar” seems to have come from an old South American Indian word, cuguacuarana, which was shortened to "cuguar" and then spelled differently. And “panther” is a general term for cats that have solid-colored coats, so it was used for black pumas as well as black jaguars and black leopards. All of these names are considered correct, but in Southern California we most commonly call them mountain lions.
You may have heard of Florida panthers. They are a subspecies of mountain lion that used to be found from Texas throughout the southeast but now only live in southern Florida’s swamps. They are Endangered, with only about 200 cats left, and conservation efforts are underway to save them.
Mountain lions are generally a solid tawny color, with slightly darker hair on their back and a whitish underside. Those living in warm, humid areas tend to be a darker, reddish-brown color, and mountain lions found in colder climates have thicker, longer hair that is almost silver-gray in color. Adult males weigh 40 to 60 percent more than adult females. Scientists classify mountain lions as small cats, as they do not roar, but purr like smaller cats do. Their slender bodies and calm demeanor are more like that of a cheetah; both cats would rather flee than fight, and both rarely confront people.
Habitat and Diet
Besides people, mountain lions have the largest range of any terrestrial mammal in the Western hemisphere, from northern British Columbia to Argentina. They live in a variety of habitats, at home in forests, prairies, deserts, and swamps—they are very adaptable cats! Mountain lions are solitary, except during breeding or when a mother is caring for her cubs. But that doesn’t mean they don’t have any contact with one another.
Mountain lions live in home ranges that vary in size from 30 to 125 square miles (7,770 to 32,375 hectares). These ranges overlap, so cats share some parts. The home range of males tends to be largest and overlap the smaller ranges of several females. Mountain lions find shelter to rest or escape from bad weather in thick brush, rocky crevices, or caves, which might be anywhere in their home range.
Although cats may see each other occasionally, they mostly leave "messages," with feces, urine, scratched logs, or marks they scrape out in the dirt or snow. Mountain lions can also growl, hiss, mew, yowl, squeak, spit, and purr to get their message across to other cats, and they are known for a short, high-pitched scream and a whistle-like call.
Mountain lions are powerfully built, with large paws and sharp claws. Their hind legs are larger and more muscular than their front legs, which gives them great jumping power. They can run fast and have a flexible spine like a cheetah’s to help them maneuver around obstacles and change direction quickly.
Even so, mountain lions are mostly ambush hunters, launching at prey to knock it off balance. They have especially keen eyesight, and they usually find prey by seeing it move. These cats may be on the prowl during the day or at night, but they are most active at dusk and dawn.
Mountain lions hunt over a large area, and it can take a week for one to travel all the way around its home range. They eat a variety of prey depending on where they live, including deer, pigs, capybaras, raccoons, armadillos, hares, and squirrels. Some larger cats even bring down prey as big as an elk or a moose. But hunting large prey brings risk, and many mountain lions suffer life-threatening injuries received from a hunt, especially from a prey’s sharp horns, antlers, or hooves. Mountain lions often bury part of their kill to save for a later meal, hiding the food with leaves, grass, dirt, or even snow, depending on the habitat and time of year.
Family Life
A female ready to breed alerts any males in the area by calling and rubbing her scent on rocks and trees. A male may stay with a female for several days before looking for his next mate. An expectant mother sets up a den where she gives birth to one to six cubs. The newborns have spots, which may help them blend in with grass, brush, and dappled sunlight. Their mother nurses them for three months or so, but they can eat meat at about six weeks of age. At six months old, their spots begin to fade, and they learn to hunt. They continue to live with their mother until they're 12 to 18 months old.
Conservation
As more people have moved into mountain lion territory, the number of encounters with them has increased. This is often "big news" and frightens people. But overall, meeting a mountain lion is an unlikely event. Mountain lions don’t want to confront people, and they do their best to avoid us. You can avoid them, too, by not hiking alone, or at dusk and dawn when mountain lions are hunting. Make noise as you hike, and don’t leave food out around a cabin or campsite, especially at night. If you do happen across a mountain lion, never approach it—always keep a respectful distance.
When Europeans first settled in North America, mountain lions lived from coast to coast. But they soon came to be viewed as threats to livestock. By the 1940s, many states, including California, placed a bounty on mountain lions. Due in major part to the bounty system, mountain lions are now confined to the West, except for a small population in Florida. Some people continue to hunt them despite legal protections.
Mountain lions have an essential role to play in our ecosystem. They are one of the top predators, and without them, populations of deer and herbivores would become unhealthy and too large for the habitat. It’s true that mountain lions can be dangerous, and coexistence challenges should be reported to state or local wildlife organizations. But people like to live and play in or near natural habitats, so we need to understand and respect the wildlife that live there. If we take responsibility for our own actions, pets, livestock, and property, we can learn to peacefully coexist with mountain lions and appreciate their power and grace.
While globally mountain lion populations are stable, they still face threats like habitat loss and fragmentation, poaching of their prey, and retaliatory hunting. In California, mountain lions are classified as a specially protected mammal.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2708 2026-02-28 00:04:31
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2507) Swallow
Gist
A swallow is a small, agile bird from the family Hirundinidae, known for its aerial acrobatics, glossy blue-black backs, red throats, and long forked tails with streamers, spending most of its time catching insects in flight, building mud nests, and migrating long distances to warmer climates for winter.
Unlike Swifts, Swallows rarely venture into towns, preferring open countryside where flying insects are plentiful. They can often be seen around open water too. As autumn approaches, large groups of Swallows often congregate on overhead wires and in reedbeds before heading south, back to Africa.
Summary
Swallow is any of the approximately 90 species of the bird family Hirundinidae (order Passeriformes). A few, including the bank swallow, are called martins (see martin; see also woodswallow; for sea swallow, see tern). Swallows are small, with pointed narrow wings, short bills, and small weak feet; some species have forked tails. Plumage may be plain or marked with metallic blue or green; the sexes look alike in most species.
Swallows spend much time in the air, capturing insects; they are among the most agile of passerine birds. For nesting, swallows may use a hole or cranny in a tree, burrow into a sandbank, or plaster mud onto a wall or ledge to house three to seven white, sometimes speckled, eggs.
Swallows occur worldwide except in the coldest regions and remotest islands. Temperate-zone species include long-distance migrants. The common swallow (Hirundo rustica) is almost worldwide in migration; an American species, called barn swallow, may summer in Canada and winter in Argentina. The 10 species of Petrochelidon, which make flask-shaped mud nests, include the cliff swallow (P. pyrrhonota), the bird of San Juan Capistrano Mission, in California; as with other swallows, it has strong homing instincts.
Details
The swallows, martins, and saw-wings, or Hirundinidae, are a family of passerine songbirds found around the world on all continents, including occasionally in Antarctica. Highly adapted to aerial feeding, they have a distinctive appearance. The term "swallow" is used as the common name for Hirundo rustica in the United Kingdom and Ireland. Around 90 species of Hirundinidae are known, divided into 21 genera, with the greatest diversity found in Africa, which is also thought to be where they evolved as hole-nesters. They also occur on a number of oceanic islands. A number of European and North American species are long-distance migrants; by contrast, the West and South African swallows are nonmigratory.
This family comprises two subfamilies: Pseudochelidoninae (the river martins of the genus Pseudochelidon) and Hirundininae (all other swallows, martins, and saw-wings). In the Old World, the name "martin" tends to be used for the squarer-tailed species, and the name "swallow" for the more fork-tailed species; however, this distinction does not represent a real evolutionary separation. In the New World, "martin" is reserved for members of the genus Progne. (These two systems are responsible for the same species being called sand martin in the Old World and bank swallow in the New World.)
Taxonomy and systematics
The family Hirundinidae was introduced (as Hirundia) by the French polymath Constantine Samuel Rafinesque in 1815. The Hirundinidae are morphologically unique within the passerines, with molecular evidence placing them as a distinctive lineage within the Sylvioidea (Old World warblers and relatives). Phylogenetic analysis has shown that the family Hirundinidae is sister to the cupwings in the family Pnoepygidae. The two families diverged in the early Miocene around 22 million years ago.
Within the family, a clear division exists between the two subfamilies, the Pseudochelidoninae, which are composed of the two species of river martins, and the Hirundininae, into which the remaining species are placed. The division of the Hirundininae has been the source of much discussion, with various taxonomists variously splitting them into as many as 24 genera and lumping them into just 12. Some agreement exists that three core groups occur within the Hirundininae: the saw-wings of the genus Psalidoprocne, the core martins, and the swallows of the genus Hirundo and their allies. The saw-wings are the most basal of the three, with the other two clades being sister to each other. The phylogeny of the swallows is closely related to evolution of nest construction; the more basal saw-wings use burrows as nest, the core martins have both burrowing (in the Old World members) and cavity adoption (in New World members) as strategies, and the genus Hirundo and its allies use mud nests.
Fossil record
The oldest known fossil swallow is Miochelidon eschata from the Early Miocene of Siberia; it is the only record of Hirundinidae from the Miocene. It is likely a basal member of the family.
Description
The Hirundinidae have an evolutionarily conservative body shape, which is similar across the clade, but is unlike that of other passerines. Swallows have adapted to hunting insects on the wing by developing a slender, streamlined body and long, pointed wings, which allow great maneuverability and endurance, as well as frequent periods of gliding. Their body shapes allow for very efficient flight; the metabolic rate of swallows in flight is 49–72% lower than equivalent passerines of the same size.
Swallows have two foveae in each eye, giving them sharp lateral and frontal vision to help track prey. They also have relatively long eyes, with their length almost equaling their width. The long eyes allow for an increase in visual acuity without competing with the brain for space inside of the head. The morphology of the eye in swallows is similar to that of a raptor.
Like the unrelated swifts and nightjars, which hunt in a similar way, they have short bills, but strong jaws and a wide gape. Their body lengths range from about 10–24 cm (3.9–9.4 in) and their weight from about 10–60 g (0.35–2.12 oz). The smallest species by weight may be the Fanti sawwing, at a mean body mass of 9.4 g (0.33 oz) while the purple martin and southern martin, which both weigh in excess of 50 g (1.8 oz) on average, rival one another as the heaviest swallows. The wings are long, pointed, and have nine primary feathers. The tail has 12 feathers and may be deeply forked, somewhat indented, or square-ended. A long tail increases maneuverability, and may also function as a sexual adornment, since the tail is frequently longer in males. In barn swallows, the tail of the male is 18% longer than those of the female, and females select mates on the basis of tail length.
Their legs are short, and their feet are adapted for perching rather than walking, as the front toes are partially joined at the base. Swallows are capable of walking and even running, but they do so with a shuffling, waddling gait. The leg muscles of the river martins (Pseudochelidon) are stronger and more robust than those of other swallows. The river martins have other characteristics that separate them from the other swallows. The structure of the syrinx is substantially different between the two subfamilies; and in most swallows, the bill, legs, and feet are dark brown or black, but in the river martins, the bill is orange-red and the legs and feet are pink.
The most common hirundine plumage is glossy dark blue or green above and plain or streaked underparts, often white or rufous. Species that burrow or live in dry or mountainous areas are often matte brown above (e.g. sand martin and crag martin). The sexes show limited or no sexual dimorphism, with longer outer tail feathers in the adult male probably being the most common distinction.
The chicks hatch naked and with closed eyes. Fledged juveniles usually appear as duller versions of the adult.
Additional Information:
About
The swallow, or 'barn swallow', is a common summer visitor, arriving in April and leaving in October. It builds mud and straw nests on ledges, often in farm buildings and outhouses, or under the eaves of houses. Swallows are widespread and common birds of farmland and open pasture near water. They are agile fliers, feeding on flying insects while on the wing. Before they migrate back to their wintering grounds in Africa, they can be seen gathering to roost in wetlands, particularly reedbeds.
How to identify
The swallow is a glossy, dark blue-black above and white below, with a dark red forehead and throat, and a black band across its chest. It has a very long, forked tail. Often spotted perching on wires in small numbers.
Distribution
Widespread.
Did you know?
Until the 19th century, people thought that the swallow hibernated over winter. Of course, we now know that it migrates to South Africa from the UK, undertaking a perilous journey, during which it is vulnerable to starvation and stormy weather.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2709 2026-03-01 00:01:44
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2508) Firefly
Gist
Light production in fireflies is due to the chemical process of bioluminescence. This occurs in specialized light-emitting organs (known as photophores), usually located on a female firefly's lower abdomen.
Summary
The Lampyridae are a family of elateroid beetles with more than 2,400 described species, many of which are light-emitting. They are soft-bodied beetles commonly called fireflies, lightning bugs, starflies or glowworms for their conspicuous production of light, mainly during twilight, to attract mates. The type species is Lampyris noctiluca, the common glow-worm of Europe. Light production in the Lampyridae is thought to have originated as a warning signal that the larvae were distasteful. This ability to create light was then co-opted as a mating signal and, in a further development, adult female fireflies of the genus Photuris mimic the flash pattern of the Photinus beetle to trap their males as prey.
Fireflies are found in temperate and tropical climates. Many live in marshes or in wet, wooded areas where their larvae have abundant sources of food. Although all fireflies nominally glow as larvae, only some species produce light in their adult stage, and the location of the light organ varies among species and between sexes of the same species. Fireflies have attracted human attention since classical antiquity; their presence has been taken to signify a wide variety of conditions in different cultures and is especially appreciated aesthetically in Japan, where parks are set aside for this specific purpose.
Firefly, (family Lampyridae) is a family of some 2,000 species of beetles (insect order Coleoptera) found in most tropical and temperate regions that have special light-producing organs on the underside of the abdomen. Most fireflies are nocturnal, although some species are diurnal. They are soft-bodied beetles that range from 5 to 25 mm (up to 1 inch) in length. The flattened, dark brown or black body is often marked with orange or yellow.
Some adult fireflies do not eat, whereas many feed on pollen and nectar. In a few species females are predatory on males of other firefly species. Both sexes are usually winged and luminous, although in some species only one sex has the light-producing organ. Females lacking wings and resembling the long, flat larvae are commonly referred to as glowworms. The larvae are sometimes luminescent before they hatch. Larvae live on the ground and feed on snails and slugs by injecting a fluid into their prey and then withdrawing the partly digested matter through hollow mouthparts. The common glowworm (Lampyris noctiluca) is a member of this family.
Most fireflies produce short, rhythmic flashes in a pattern characteristic of the species. The rhythmic flash pattern is part of a signal system that brings the sexes together. Both the rate of flashing and the amount of time before the female’s response to the male are important. Some authorities feel that the flashing is also a protective mechanism, reminding predators of the firefly’s bitter taste. However, some frogs eat such large numbers of fireflies that they themselves glow.
Firefly light is produced under nervous control within special cells (photocytes) richly supplied with air tubes (tracheae). Firefly light is a cold light with approximately 100 percent of the energy given off as light and only a minute amount of heat. Only light in the visible spectrum is emitted. Some tropical members of the coleopteran family Elateridae are also called fireflies.
The emitted light (due to a chemical process known as bioluminescence) of such organisms as fireflies, various marine organisms (see marine bioluminescence), and a number of algae, fungi, and bacteria is based on the oxidation of any of several organic molecules known as luciferins. The luciferins are broken down by the enzyme luciferase and react with the energy molecule ATP and oxygen, resulting in a glowing light.
Details
It’s a quiet, warm summer evening with no human in sight for miles in the woods. As the sun sets, tiny flashes of light start to flicker throughout the trees. At first there’s just a few, but soon hundreds of blinking lights are floating in the forest. Fireflies have come out for the evening.
Flying Beetles
Also known as lightning bugs, fireflies are beetles. Most fireflies are winged. That’s different from other light-producing insects of the same family, called glowworms. (Animals that produce light are called luminescent.)
There are about 2,000 firefly species. These insects often live in humid regions of Asia and the Americas, where they mostly feast on plant pollen and nectar. Firefly larvae—recently hatched worm-like fireflies that haven’t fully developed yet (including their wings)—feed on worms, snails, and insects.
You Glow, Guys!
Fireflies mostly use their light to “talk” to other fireflies and find a mate. They have special organs under their abdomens that take in oxygen. Inside special cells, they combine the oxygen with a substance called luciferin to make light with almost no heat. They use this light, called bioluminescence, to light up the ends of their abdomen.
Each firefly species has its own unique flashing pattern. When a male firefly wants to communicate with a female firefly, he flies near the ground while he flashes his light every six seconds. Once he’s near the ground, a female can more easily tell if he’s from the same species as she is. (Most female fireflies can’t fly.) She answers his flashes by turning on her lights. Then the male finds her.
Predators, such as birds or toads, get a different message from these lights. Although they can easily spot fireflies by their glow, they rarely eat them. That’s because fireflies release drops of toxic, foul-tasting blood. Their flashing is a warning light to predators to stay away.
Lights Out?
Fireflies aren’t endangered, but scientists are worried about them. In recent years, fewer of the insects have been spotted during the summer. Pesticide use and loss of habitat have likely impacted the population, as has light pollution. Too much nighttime light can be harmful to wildlife, affecting their migration patterns and hunting abilities. For fireflies, light pollution interferes with their attempts to signal each other.
Scientists aren’t sure how much the firefly population has dropped since their small size makes them hard to tag and track. Plus an adult firefly's life span is just one to three weeks, which makes counting them difficult. Scientists are working on ways to better track and protect these insects.
Additional Information
Scientifically, fireflies are classified under Lampyridae, a family of insects within the beetle order Coleoptera, or winged beetles. There are estimated to be 2000+ firefly species spread across temperate and tropical zones all over the world.
Hear the word firefly or lightningbug, and what comes to mind? Warm summer nights? Flickering lights in the encroaching dark? Maybe soft grass underfoot, with children running about? Few species ignite such warm feelings of nostalgia as fireflies. These beacons of light are some of our most beloved insects, and no wonder. Their bioluminescence fills us with awe. Their very presence feels magical. Their light has inspired artwork, literature, dance, and music. Beyond their immense cultural value, they have played critical roles in scientific research and medicine, and they are integral components of healthy, thriving ecosystems.
Fireflies are cherished, but they are also declining. Anecdotal reports from around the globe describe fewer individuals being seen each year. And while long-term monitoring studies are scarce, some of the data we have are concerning. For example, based on assessments published on the International Union for Conservation of Nature’s (IUCN) Red List of Threatened Species, one in three assessed North American fireflies may be at risk of extinction. Researchers found that 14% of the assessed species were categorized as threatened, but this number may be much higher since nearly half of the assessed species are data deficient. There is an urgent need to study firefly populations more closely to fully understand their plight and ensure conservation efforts are effective.
Introduction
In many places the insects called fireflies are a familiar sight on summer nights. They are noticeable because they can produce flashes of light. Fireflies belong to the beetle family. They are also called lightning bugs.
Where Fireflies Live
There are about 2,000 species, or types, of firefly. They live in tropical and mild parts of the world. They generally like warm, humid areas, but some live in dry places.
Fireflies retire into the ground during the day. At night, they tend to flock to dark, open areas where their lights can be the most noticeable. The best time to see them is in the later evening hours on dry summer nights.
Physical Features
Adult fireflies range in size from 0.2 to 1 inch (5 to 25 millimeters) long. They have a soft, flattened body that is dark brown or black, sometimes with orange or yellow marks. Males have wings and are good fliers. Females either have short wings or no wings. The females without wings are often called glowworms. Young fireflies, which also have no wings, are also called glowworms.
Behavior
Fireflies produce light with special organs, or body parts, on the underside of the body. These organs make light by mixing chemicals with oxygen from the air. Fireflies make a certain series of flashes to attract a mate. When a possible mate sees the flashes, it returns the signal.
Life Cycle
Females die soon after laying eggs, which hatch into larvae within a few weeks. It takes larvae one or two summers to grow into adults. Larvae can glow, but much more faintly than adults and only for a few seconds at a time. Larvae eat tiny snails and slugs, but adult fireflies may not eat.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2710 2026-03-02 00:03:08
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2509) Refrigerant
Gist
Refrigerants are chemical fluids (compounds) used in HVAC and refrigeration systems that alternate between liquid and gaseous states to absorb, transport, and release heat, thereby cooling spaces or items. Common types include Hydrofluorocarbons (HFCs like R-134a, R-410A) and increasingly, eco-friendly natural refrigerants like propane and CO2.
Refrigerant is the working fluid used in air conditioners, refrigeration, and heat pump systems. It is a chemical compound that changes temperature as it transitions between liquid and gas form – cooling as it vaporizes, and heating up as it condenses.
Summary
Refrigerants are working fluids that carry heat from a cold environment to a warm environment while circulating between them. For example, the refrigerant in an air conditioner carries heat from a cool indoor environment to a hotter outdoor environment. Similarly, the refrigerant in a kitchen refrigerator carries heat from the inside the refrigerator out to the surrounding room. A wide range of fluids are used as refrigerants, with the specific choice depending on the temperature range needed and constraints related to the system involved.
Refrigerants are the basis of vapor compression refrigeration systems. The refrigerant is circulated in a loop between the cold and warm environments. In the low-temperature environment, the refrigerant absorbs heat at low pressure, causing it to evaporate. The gaseous refrigerant then enters a compressor, which raises its pressure and temperature. The pressurized refrigerant circulates through the warm environment, where it releases heat and condenses to liquid form. The high-pressure liquid is then depressurized and returned to the cold environment as a liquid-vapor mixture.
Refrigerants are also used in heat pumps, which work like refrigeration systems. In the winter, a heat pump absorbs heat from the cold outdoor environment and releases it into the warm indoor environment. In summer, the direction of heat transfer is reversed.
Refrigerants include naturally occurring fluids, such as ammonia, carbon dioxide, propane, or isobutane, and synthetic fluids, such as chlorofluorocarbons, hydrochlorofluorocarbons, or hydrofluorocarbons. Many older synthetic refrigerants have been banned to protect the Earth's ozone layer or to limit climate change. Some refrigerants are flammable or toxic, making careful handling and disposal essential.
Refrigerants, while strongly associated with vapor compression systems, are used for many other purposes. These applications include propelling aerosols, polymer foam production, chemical feedstocks, fire suppression, and solvents.
Chillers are refrigeration systems that have a secondary loop which circulates a refrigerating liquid (as opposed to a refrigerant), with vapor compression refrigeration used to chill the secondary liquid.[5] Absorption refrigeration systems operate by absorbing a gas, such as ammonia, into a liquid, such as water.
Details
Refrigerants are crucial for commercial refrigeration systems, responsible for cooling and preserving perishable items. With refrigerant regulations phasing out ozone-depleting refrigerants, such as R-22, many businesses are transitioning to more environmentally friendly options. Understanding the different types of refrigerants available for commercial use can help you make an informed decision when it comes to replacing your refrigerator or freezer.
What Is Refrigerant?
Refrigerant is a cooling agent that absorbs heat and leaves cool air behind when passed through a compressor and evaporator. It undergoes a continuous cycle of compression and expansion where the coolant fluctuates between a liquid or gas state as it goes through the thermodynamic process to transfer heat efficiently.
How Refrigerant Works
Here is how refrigerant cools the inside of refrigerators and the air for AC units:
1) The refrigerant begins as a liquid when it passes through the expansion device in your unit. It expands and cools due to the sudden drop in pressure causing it to turn into a gas.
2) As the gaseous refrigerant passes through the copper evaporator coil inside the unit, it absorbs the heat from the products inside.
3) The unit’s compressor then pulls the refrigerant gas and the absorbed heat away from the food products, increasing the pressure of the gas.
4) The hot, high-pressure refrigerant then passes through the condenser coils. As it does so, it radiates its heat into the atmosphere and cools back into a liquid.
5) The liquid refrigerant reenters the expansion device and the process begins again.
Types of Refrigerant
Common types of refrigerants include synthetic compounds like hydrofluorocarbons (HFCs), hydrochlorofluorocarbons (HCFCs), and natural compounds like ammonia and carbon dioxide. Each type has its own unique ID number, properties, and environmental impact, making it important for businesses to choose the right refrigerant for their specific needs.
Because of the negative impact on the environment, there are refrigerant regulations in place that have listed a variety of banned refrigerant types that are being phased out and replaced with more environmentally friendly alternatives. A refrigerant’s environmental impact is measured by two main characteristics: Ozone Depletion Potential (ODP) and Global Warming Potential (GWP). ODP measures a refrigerant's impact on the ozone layer, while GWP assesses its contribution to global warming. Choosing refrigerants with lower ODP and GWP values can help businesses reduce their environmental footprint and comply with regulations aimed at mitigating climate change.
Additional Information
When we say “refrigerant” we mean a fluid that can easily boil from a liquid into a vapour and also be condensed from a vapour back into a liquid. This needs to occur again and again, continuously without fail.
An example of a refrigerant would be water. This is able to evaporate and condense and is easy and safe to use. It’s used in Absorption chillers as a refrigerant, you can find out more about this type of chiller by clicking here. The reason water isn’t typically used as a refrigerant in common air conditioning units is because there are specially made refrigerants designed specifically for this task, and these are able to perform much more efficiently.
Some of the more common refrigerants on the market ate R22, R134A and R410A, although the laws and regulations on refrigerants are tightening and many of these will be phased out in the long run. These common refrigerants all have extremely low boiling points compared to water. This allows it to evaporate into a vapour with very little thermal energy applied which means the refrigerant can extract heat more rapidly.
Lets look at how refrigerant moves around the system. We’ll start with the compressor as this is the heart of the system, it forces the refrigerant around each of the components within the refrigeration system. The refrigerant will enter as a saturated vapour and is a low temperature and low pressure. As the compressor pulls the refrigerant in, it rapidly compresses it, this forces the molecules together so the same amount of molecules fits into a smaller volume. The molecules are all constantly bouncing around and compressing them into a smaller space causes them to collide more often, as they collide they convert their kinetic energy into heat. At the same time, all the energy that is put in by the compressor is converted into internal energy within the refrigerant. This results in the refrigerant increasing in internal energy, enthalpy, temperature and pressure. You’ll know this if you’ve ever used a bike pump, the pump becomes very hot as the pressure increases.
The refrigerant now moves to the condenser. The condenser is where all the unwanted heat is rejected out into the atmosphere. This will include all the heat from the building as well as the heat from the compressor. When the refrigerant enters the condenser, it needs to be at a higher temperature than the ambient air around it, in order for the heat to transfer. The greater the temperature difference, the easier the heat transfer will be. The refrigerant enters as a superheated vapour at high pressure and temperature, it then passes along the tubes of the condenser. During this move, fans will blow air across the condenser (in an air cooled system) to remove the unwanted energy. Much like blowing a hot spoon of soup to cool it down. As the air blows across the tubes, it removes heat from the refrigerant. As the refrigerant gives up its heat it will condense into a liquid so by the time the refrigerant leaves the condenser it will be a completely saturated liquid, still at high pressure, but slightly cooler although it will have decreased in both enthalpy and entropy.
The refrigerant then makes its way to the expansion valve. The expansion valve meters the flow of refrigerant into the evaporator. In this example we’re using a thermal expansion valve which holds back refrigerant, creating a high and low pressure side. The valve will then adjust to allow some refrigerant to flow and this will be part liquid and part vapour. As it passes through it will expand to try and fill the void. As it expands the refrigerant reduces in pressure and temperature, just like if you hold a deodorant spray can and hold the trigger down. The refrigerant leaves the expansion valve at low pressure and temperature then heads straight into the evaporator.
The evaporator receives the refrigerant and another fan blows the warm air of the room across the evaporator coil. The temperature of the room air is higher than the temperature of the cool refrigerant this allows it to absorb more energy and boil the refrigerant completely into a vapour. Much like heating a pan of water, the heat will cause the water to evaporate into steam vapour and the vapour will carry the heat away, if you were to place your hand over the rising steam you will find it’s very hot. Although I wouldn’t recommend this and it can cause injury. Remember we looked earlier at the low boiling point of refrigerants, so room temperature air is enough to boil it into a vapour.
The refrigerant leaves the evaporator as a low temperature, low pressure vapour. The temperature only changes slightly which confuses many people, but the reason it doesn’t increase dramatically is because it is undergoing a phase change from a liquid to a vapour so the thermal energy is being used to break the bonds between the molecules but the enthalpy and entropy will increase and this is where the energy is going. The temperature will only change once the fluid is no longer undergoing a phase change.
1. The expansion valve relieves pressure and passes the refrigerant into the evaporator coil as a cold, low-pressure liquid.
2. As the refrigerant warms within the coil, it phases back into a gaseous state.
3. The cool gas is compressed and fed into the condenser coil as a hot, high-pressure gas.
4. As the hot, pressurized refrigerant cools within the condenser coil, it phases back into a warm liquid state.
5. This process triggers the air handler within your system to distribute the heated or cooled air throughout your home based on your thermostat settings.
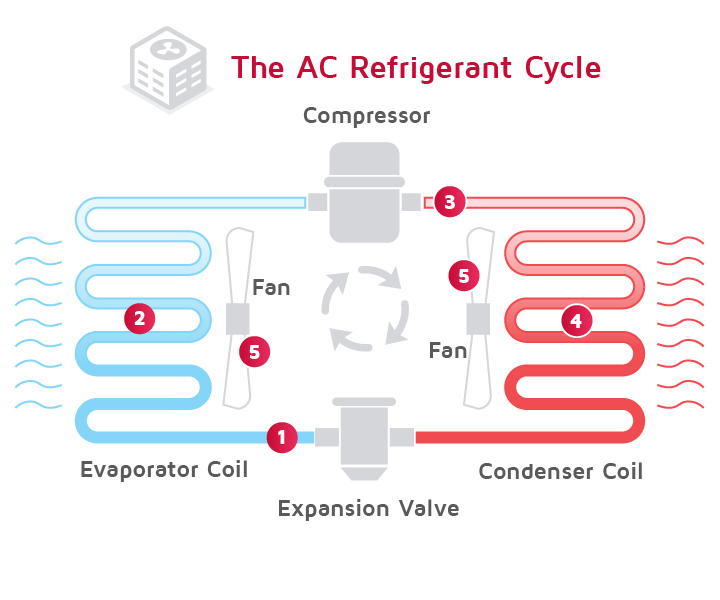
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2711 2026-03-03 00:06:27
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2510) Glaucoma
Gist
Glaucoma is a group of eye conditions that damage the optic nerve, often due to high eye pressure, potentially causing permanent blindness. Known as the "silent thief of sight," it usually has no early symptoms until significant vision loss occurs. Treatments include medicated eye drops, laser therapy, or surgery to lower pressure.
The main cause of glaucoma is damage to the optic nerve, often linked to increased pressure inside the eye (intraocular pressure or IOP) from fluid buildup, but it can also occur with normal pressure due to poor blood flow or other factors, with genetics, age, eye injury, and conditions like diabetes being significant risk factors. This damage happens when the eye's drainage system, the trabecular meshwork, doesn't work correctly, causing fluid (aqueous humor) to build up, press on the optic nerve, and impair vision.
Summary
Your eye constantly makes aqueous humor. As new aqueous flows into your eye, the same amount should drain out. The fluid drains out through an area called the drainage angle. This process keeps pressure in the eye (called intraocular pressure or IOP) stable. But if the drainage angle is not working properly, fluid builds up. Pressure inside the eye rises, damaging the optic nerve.
The optic nerve is made of more than a million tiny nerve fibers. It is like an electric cable made up of many small wires. As these nerve fibers die, you will develop blind spots in your vision. You may not notice these blind spots until most of your optic nerve fibers have died. If all of the fibers die, you will become blind.
How Do You Get Glaucoma?
There are two major types of glaucoma.
Open-angle glaucoma
This is the most common type of glaucoma. It happens gradually, where the eye does not drain fluid as well as it should (like a clogged drain). As a result, eye pressure builds and starts to damage the optic nerve. This type of glaucoma is painless and causes no vision changes at first.
Some people can have optic nerves that are sensitive to normal eye pressure. This means their risk of getting glaucoma is higher than normal. Regular eye exams are important to find early signs of damage to their optic nerve.
Angle-closure glaucoma (also called “closed-angle glaucoma” or “narrow-angle glaucoma”)
This type happens when someone’s iris is very close to the drainage angle in their eye. The iris can end up blocking the drainage angle. You can think of it like a piece of paper sliding over a sink drain. When the drainage angle gets completely blocked, eye pressure rises very quickly. This is called an acute attack. It is a true eye emergency, and you should call your ophthalmologist right away or you might go blind.
Here are the signs of an acute angle-closure glaucoma attack:
* Your vision is suddenly blurry
* You have severe eye pain
* You have a headache
* You feel sick to your stomach (nausea)
* You throw up (vomit)
* You see rainbow-colored rings or halos around lights
Many people with angle-closure glaucoma develop it slowly. This is called chronic angle-closure glaucoma. There are no symptoms at first, so they don’t know they have it until the damage is severe or they have an attack.
Angle-closure glaucoma can cause blindness if not treated right away.
Details
Glaucoma is a group of eye diseases that can lead to damage of the optic nerve, which transmits visual information from the eye to the brain. Glaucoma may cause vision loss if left untreated. It has been called the "silent thief of sight" because the loss of vision usually occurs slowly over a long period of time. A major risk factor for glaucoma is increased pressure within the eye, known as intraocular pressure (IOP). It is associated with old age, a family history of glaucoma, and certain medical conditions or the use of some medications.[6] The word glaucoma comes from the Ancient Greek word (glaukós), meaning 'gleaming, blue-green, gray'.
Of the different types of glaucoma, the most common are called open-angle glaucoma and closed-angle glaucoma. Inside the eye, a liquid called aqueous humor, which is produced by the ciliary body, helps to maintain shape and provides nutrients. The aqueous humor normally drains through the trabecular meshwork. In open-angle glaucoma, the drainage is impeded, causing the build up of aqueous to accumulate in the anterior chamber causing the pressure inside the eye to increase. This elevated pressure can reduce vascular perfusion in the vitreous chamber and can damage the optic nerve and peripheral glial tissues. In closed-angle glaucoma, the drainage of the eye becomes suddenly blocked, leading to a rapid increase in intraocular pressure. This may lead to intense eye pain, blurred vision, and nausea. Closed-angle glaucoma is an emergency requiring immediate attention.
If treated early, the progression of glaucoma may be slowed or even stopped. Regular eye examinations, especially if the person is over 40 or has a family history of glaucoma, are essential for early detection. Treatment typically includes prescription of eye drops, medication, laser treatment or surgery. The goal of these treatments is to decrease eye pressure.
Glaucoma is a leading cause of blindness in African Americans, Hispanic Americans, and Asians. Its incidence rises with age, to more than eight percent of Americans over the age of eighty, and closed-angle glaucoma is more common in women.
Additional Information
Glaucoma refers to many diseases involving eye pressure increases that lead to permanent vision loss and blindness. This condition can happen for many reasons, but most are treatable. Knowing the risk factors and getting regular eye exams may help you avoid vision loss.
Overview:
What is glaucoma?
Glaucoma is an umbrella term for eye diseases that make pressure build up inside your eyeball, which can damage delicate, critical parts at the back of your eye. Most of these diseases are progressive, which means they gradually get worse. As they do, they can eventually cause permanent vision loss and blindness. In fact, glaucoma is the second-leading cause of blindness worldwide.
Learning that you have glaucoma or that you’re at risk for it can be hard to process. For most people, vision is the sense they rely on most in their daily routine. It can feel scary to imagine trying to adapt to and live your life after you have severe vision loss. But most forms of glaucoma are treatable, especially when diagnosed early. And with care and careful management, it’s possible to delay — or even prevent — permanent vision loss.
Symptoms and Causes:
What are the symptoms of glaucoma?
In its early stages, glaucoma may not cause any symptoms. That’s why up to half of the people in the United States with glaucoma may not know they have it. And symptoms may not appear until this condition causes irreversible damage.
Some of the more common glaucoma symptoms include:
* Eye pain or pressure
* Headaches
* Red or bloodshot eyes
* Double vision (diplopia)
* Blurred vision
* Gradually developing low vision
* Gradually developing blind spots (scotomas) or visual field defects like tunnel vision
Some types of glaucoma, particularly angle closure glaucoma, can cause sudden, severe symptoms that need immediate medical attention to prevent permanent vision loss. Emergency glaucoma symptoms include:
* Blood gathering in front of your iris (hyphema)
* Bulging or enlarged eyeballs (buphthalmos)
* Nausea and vomiting that happen with eye pain/pressure
* Rainbow-colored halos around lights
* Sudden appearance or increase in floaters (myodesopsias)
* Sudden vision loss of any kind
* Suddenly seeing flashing lights (photopsias) in your vision
What causes glaucoma?
Glaucoma is caused by damage to your optic nerve. It can occur without any cause, but many factors can affect the condition. The most important of these risk factors is intraocular eye pressure. Your eyes produce a fluid called aqueous humor that nourishes them. This liquid flows through your pupil to the front of your eye. In a healthy eye, the fluid drains through mesh-like canals (trabecular meshwork), which is where your iris and cornea come together at an angle.
With glaucoma, the resistance increases in your drainage canals. The fluid has nowhere to go, so it builds up in your eye. This excess fluid puts pressure on your eye. Eventually, this elevated eye pressure can damage your optic nerve and lead to glaucoma.
What makes the fluid build up can vary, depending on the specific overall type of glaucoma you have.
Types of glaucoma
There are many different types of glaucoma, but they mainly fall under a few specific categories:
* Primary open-angle glaucoma. “Open-angle” means that the drainage angle, where the inside of the sclera (the white of your eye) and the outer edge of your iris meet, is open wide. Aqueous humor flows into the drainage angle so it can drain out of the anterior chamber. This is the most common type of glaucoma.
* Primary angle-closure glaucoma. Aqueous humor fluid is supposed to flow from the posterior chamber behind your iris, through your pupil, and into the anterior chamber. But sometimes, the lens of your eye presses too far forward, blocking fluid from flowing through the pupil opening. The extra fluid in the posterior chamber forces the iris forward, narrowing or closing off the drainage angle.
* Secondary glaucoma. This is when another condition or event increases eye pressure, which leads to glaucoma. Conditions that can cause it include eye injuries, pigmentary dispersion syndrome, uveitis, certain medications (especially corticosteroids and cycloplegics), eye procedures and more.
* Congenital glaucoma. This means you have glaucoma because of changes or differences that happened during fetal development. These include aniridia, Axenfeld-Rieger syndrome, Marfan syndrome, congenital rubella syndrome and neurofibromatosis type 1.
What are the risk factors for glaucoma?
Several risk factors can contribute to glaucoma. They include:
* Age. Most types of glaucoma affect people age 40 and older (congenital types are the biggest exception to this). Experts estimate that 10% of people age 75 and older have glaucoma.
* Race. Black people have a much higher risk of developing primary open-angle glaucoma, especially people of Afro-Caribbean descent. People of African descent are 15 times more likely to have blindness from open-angle glaucoma. People of Asian and Inuit descent have a higher risk of angle-closure glaucoma.
* sex. Women have a higher risk of angle-closure glaucoma. Experts suspect this is mainly because of sex-linked differences in eye anatomy.
* Refractive errors. People with nearsightedness (myopia) have a higher risk of open-angle glaucoma. People with farsightedness (hyperopia) have a higher risk of angle-closure glaucoma.
* Family history. There’s evidence that a family history of glaucoma, especially a first-degree biological relative (a parent, child or sibling), means you also have a higher risk of developing it. And several conditions that cause secondary glaucoma are genetic, too.
* Chronic conditions. Research links some conditions, like high blood pressure (hypertension) and diabetes, to much higher odds of developing glaucoma.
What are the complications of glaucoma?
Without care to manage it and lower the pressure inside your eye, glaucoma damages your retina and optic nerve to the point where they stop working. That causes glaucoma’s main complication: vision loss and, eventually, total blindness.
The end result is what experts call “absolute glaucoma.” That means you’re totally blind in the affected eye. The affected eye feels hard — and maybe even painful — when you touch it.
Diagnosis and Tests:
How is glaucoma diagnosed?
An eye care specialist can diagnose glaucoma using an eye exam, including several tests that are part of routine eye exams. In fact, eye exams can detect glaucoma long before you have eye damage and the symptoms that follow. Many of these tests involve pupil dilation (mydriasis), so your provider can get a better look inside your eye.
Some of the most helpful glaucoma tests include:
* Visual acuity testing
* Visual field testing
* Depth perception testing
* Tonometry
* Pachymetry
* Slit lamp exam
* Gonioscopy
If your eye care specialist has a reason to suspect damage to your retina and/or optic nerve, they may also use additional types of eye imaging. These include:
* Optical coherence tomography
* Fluorescein angiography
* Ultrasound
* Less commonly, computed tomography (CT) or magnetic resonance imaging (MRI).
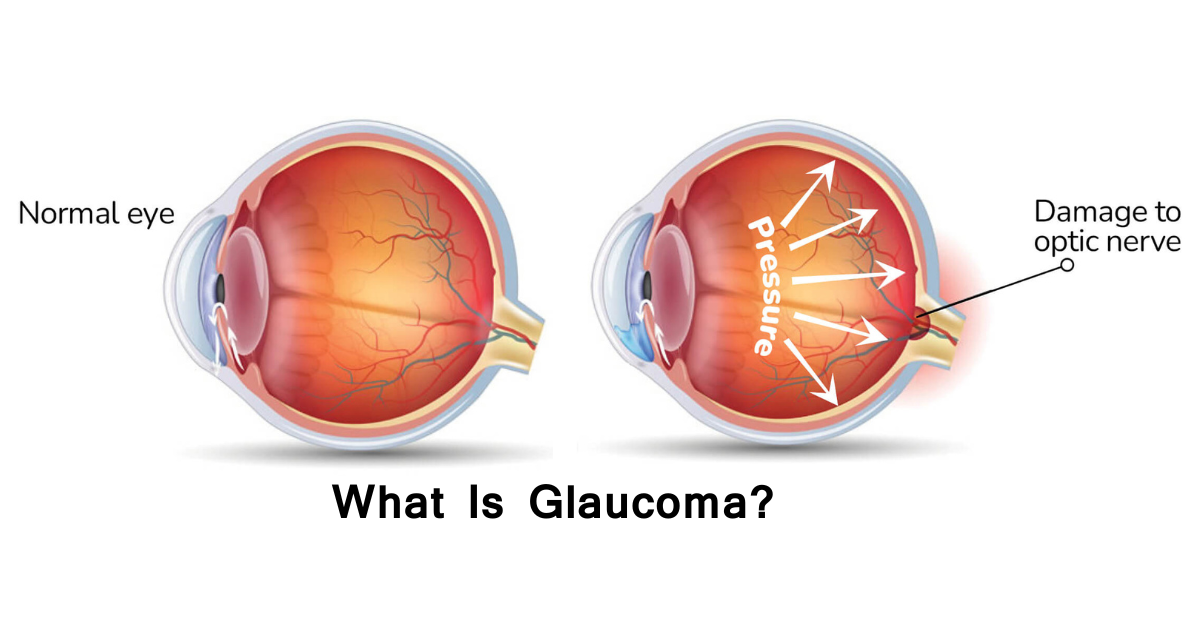
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2712 2026-03-04 00:03:17
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2511) Tonometry
Gist
Tonometry is a quick, non-invasive diagnostic procedure that measures intraocular pressure (IOP), or fluid pressure inside the eye, to detect and monitor glaucoma. By assessing how much force is needed to flatten the cornea (applanation) or indent it, doctors can check for optic nerve damage. The most common methodGoldmann applanation tonometry, is considered the gold standard.
How is tonometry performed?
The lamp is moved forward until the tip of the tonometer just touches the cornea. Blue light is used so that the orange dye will glow green. The health care provider looks through the eyepiece on the slit-lamp and adjusts a dial on the machine to give the pressure reading. There is no discomfort with the test.
Summary
A tonometry test measures the pressure inside your eye, which is called intraocular pressure (IOP). This test is used to check for glaucoma, an eye disease that can cause blindness by damaging the nerve in the back of the eye (optic nerve). Damage to the optic nerve may be caused by a buildup of fluid that does not drain properly out of the eye.
Tonometry measures IOP by recording the resistance of your cornea to pressure (indentation). Eyedrops to numb the surface of your eye are used with most of the following methods.
Tonometry methods
* Applanation (Goldmann) tonometry. This type of tonometry uses a small probe to gently flatten part of your cornea to measure eye pressure and a microscope called a slit lamp to look at your eye. The pressure in your eye is measured by how much force is needed to flatten your cornea. This type of tonometry is very accurate and is often used to measure IOP after a simple screening test (such as air-puff tonometry) finds an increased IOP.
* Electronic indentation tonometry. Electronic tonometry is being used more often to check for increased IOP. Although it is very accurate, electronic tonometry results can be different than applanation tonometry. Your doctor gently places the rounded tip of a tool that looks like a pen directly on your cornea. The IOP reading shows on a small computer panel.
* Noncontact tonometry (pneumotonometry). Noncontact (or air-puff) tonometry does not touch your eye but uses a puff of air to flatten your cornea. This type of tonometry is not the best way to measure intraocular pressure. But it is often used as a simple way to check for high IOP and is the easiest way to test children. This type of tonometry does not use numbing eyedrops.
Details
Tonometry is a test to measure the pressure inside your eyes. The test is used to screen for glaucoma. It is also used to measure how well glaucoma treatment is working.
How the Test is Performed
There are three main methods of measuring eye pressure.
The most accurate method measures the force needed to flatten an area of the cornea.
* The surface of the eye is numbed with eye drops. A fine strip of paper stained with orange dye is held to the side of the eye. The dye stains the front of the eye to help with the exam. Sometimes the dye is in the numbing drops.
* You will rest your chin and forehead on the support of a slit lamp so that your head is steady. You will be asked to keep your eyes open and to look straight ahead. The lamp is moved forward until the tip of the tonometer just touches the cornea.
* Blue light is used so that the orange dye will glow green. The health care provider looks through the eyepiece on the slit-lamp and adjusts a dial on the machine to give the pressure reading.
* There is no discomfort with the test.
A second method uses a handheld device shaped like a pen. You are given numbing eye drops to prevent any discomfort. The device touches the surface of the cornea and instantly records eye pressure.
The last method is the noncontact method (air puff). In this method, your chin rests on a device similar to a slit lamp.
* You stare straight into the examining device. When you are at the correct distance from the device, a tiny beam of light reflects off of your cornea onto a detector.
* When the test is performed, a puff of air will slightly flatten the cornea; how much it flattens depends on the eye pressure.
* This causes the tiny beam of light to move to a different spot on the detector. The instrument calculates eye pressure by looking at how far the beam of light moved.
How to Prepare for the Test
Remove contact lenses before the exam. The dye can permanently stain contact lenses.
Tell your provider if you have a history of corneal ulcers or eye infections, or a history of glaucoma in your family. Always tell your provider what medicines you are taking.
How the Test will Feel
If numbing eye drops were used, you should not have any pain. In the noncontact method, you may feel mild pressure on your eye for a brief moment from the air puff.
Why the Test is Performed
Tonometry is a test to measure the pressure inside your eyes. The test is used to screen for glaucoma and to measure how well glaucoma treatment is working.
People over age 40 years, particularly African Americans, have the highest risk for developing glaucoma. Regular eye exams can help detect glaucoma early. If it is detected early, glaucoma can be treated before too much damage is done.
The test may also be done before and after eye surgery.
Normal Results
A normal result means your eye pressure is within the normal range. The normal eye pressure range is 10 to 21 mm Hg.
The thickness of your cornea can affect measurements. Normal eyes with thick corneas have higher readings, and normal eyes with thin corneas have lower readings. A thin cornea with a high reading may be very abnormal (the actual eye pressure will be higher than shown on the tonometer).
A corneal thickness measurement (pachymetry) is needed to get a correct pressure measurement.
Talk to your provider about the meaning of your specific test results.
What Abnormal Results Mean
Abnormal results may be due to:
* Glaucoma
* Hyphema (blood in the front chamber of the eye)
* Inflammation in the eye
* Injury to the eye or head
* Recent eye surgery
Risks
If the applanation method is used, there is a small chance the cornea may be scratched (corneal abrasion). The scratch will normally heal within a few days.
Alternative Names
Intraocular pressure (IOP) measurement; Glaucoma test; Goldmann applanation tonometry (GAT).
Additional Information
Tonometry refers to diagnostic tests that measure your intraocular pressure (IOP), or the pressure inside your eye. There are multiple methods available, and some don’t touch your eye at all. The various test methods can help your eye care specialist detect glaucoma before it causes permanent damage and vision loss.
Overview:
What is tonometry?
Tonometry refers to a type of eye test that measures pressure inside your eye (intraocular pressure). It’s one of the essential glaucoma tests. There are a few different methods and ways to do this test, all of which are quick and painless.
When is tonometry used?
Eye care specialists, especially ophthalmologists and optometrists, use tonometry to screen for and diagnose glaucoma. It’s a common part of routine eye exams and more specific exams when you have possible eye injuries or experience certain eye symptoms.
Eye specialists may also use tonometry to monitor your eye pressure if you’re taking certain medications. Monitoring your eye pressure makes sure that those medications don’t cause high intraocular pressure (ocular hypertension) as a side effect.
If you have glaucoma, regular tonometry determines treatment. Tracking your eye pressure is a key way to make sure treatment is effective, so frequent tonometry tests — including with devices you can use at home to take readings on yourself — are common.
Test Details:
How does tonometry work?
Tonometry measures the pressure of your eye’s anterior chamber. The anterior chamber is a fluid-filled space just behind your cornea at the front of your eye. Pressure from the aqueous humor fluid inside that chamber helps your eyes hold their globe-like shape. The unit of measurement for this is millimeters of mercury (mmHg), the same unit used for blood pressure tests.
Your eye care specialist can use a few different tonometry methods. Those include:
* Applanation tonometry. “Applanation” means “flattening,” and devices that use it have a small, disk-shaped extension that rests against your eye surface. The devices measure how much pressure it takes to make your eye surface start to flatten. This method is the most accurate. It’s common for eye specialists to use this method after other methods return unusual or concerning readings.
* Continuous monitoring. This method uses a sensor you wear on your eye like a contact lens. Researchers are investigating the wearable sensor and another, similar method that uses a surgically implanted sensor.
* Dynamic contour tonometry. These devices use a small, sensor-tipped extension that touches your eye (but doesn’t make an indention).
* Electronic indentation tonometry. Devices that use this method have a small probe that takes a measurement when it presses against the surface of your eye enough to make a small indention.
* Non-contact tonometry. Devices using this method push air at your cornea. The device then measures tiny, split-second changes in the shape of your cornea as the air bounces off its surface. Air puff tonometers do this with a small puff of air, while ocular response analyzers use a stream of air.
* Rebound tonometry. Devices using this method have a tiny, plastic ball that moves toward your eye and stops when it touches the surface. The device determines your intraocular pressure when the ball makes gentle, painless contact. Some devices that use this method are ones your eye specialist can prescribe for you to take and use at home.
How should I prepare for a tonometry test?
You shouldn’t need to prepare for a tonometry test. One exception is to make sure you don’t wear a tight collar doing the test (either by wearing another shirt or loosening the collar if possible). Pressure around your neck from your clothes can increase your intraocular pressure readings.
What should I expect during a tonometry test?
What you can expect from tonometry tests can vary depending on the method. If you’re having applanation tonometry, your provider will add eye drops containing an anesthetic and a dye called fluorescein to your eyes. But non-contact tonometry and most other methods don’t need either of these to work.
Some of the most common methods for the tonometry test only take a few seconds. Many of these faster methods work best with calculating an average of multiple readings, so don’t be surprised or think you’ve done something wrong if your eye specialist wants to retake the readings a few times. Other methods (like applanation tonometry) take up to a few minutes. Your eye specialist will tell you more about what to expect during the test.
What should I expect after the test?
Your provider can tell you the reading right after they take it.
If you received anesthetic eye drops, don’t let anything touch your eyes until the anesthetic wears off. Anesthetic drops keep you from feeling pain, so it’s easier to injure your eyes while they’re numb.
Is tonometry painful?
Tonometry shouldn’t hurt, even if the method used involves touching your eyeball in some way. If you have pain during the test, tell your eye care specialist. You can also ask them more about what to expect regarding that pain, including how long it should last and what you can do about it.
Results and Follow-Up:
What is a normal tonometry range?
A normal reading for most people is 10 mmHg to 21 mmHg. If your results are outside the normal range, there are a few likely next steps.
If your results are too high
If simpler tests show high pressure, your eye specialist will probably recommend using applanation tonometry to verify the readings. If applanation tonometry confirms that your pressure is high, your provider may monitor closely or offer treatment options. They’ll want to schedule regular follow-up visits.
Your eye specialist may recommend that you test your eye pressure at home. Be sure to ask about what to do if you get readings that are outside the normal range. You may need a follow-up visit with your specialist if you get slightly higher-than-normal pressures. But, if you get much higher readings, you may need emergency medical care.
Eye pressure that’s high because of angle-closure glaucoma is a medical emergency that needs immediate treatment. Without quick treatment, angle-closure glaucoma can quickly cause eye damage and permanent vision loss.
Other next steps can vary depending on your specific situation and needs. Your eye specialist can tell you more about what you can expect for your specific case.
If your results are too low
Low intraocular pressure is also a cause for concern since it can lead to eye damage and vision loss. Low intraocular pressure is usually anything under 5 mmHg or 6 mmHg. If the pressure in your eye is too low, your eye specialist will talk to you about treatment options and follow-up visits to monitor your eye health.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2713 2026-03-05 00:03:13
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2512) Intraocular Lens
Gist
Intraocular lenses (IOLs) are tiny, artificial, permanent lenses implanted inside the eye to replace a natural lens removed during cataract surgery or to correct refractive errors like myopia, hyperopia, and astigmatism. Made of acrylic or silicone, they restore clear vision by focusing light on the retina without needing maintenance.
Intraocular lenses usually last a lifetime. How is an intraocular lens used in cataract surgery? Cataract surgery involves removing the eye's natural lens which has become cloudy (cataract) and replacing it with an intraocular lens.
Summary
An intraocular lens (or IOL) is a tiny, artificial lens for the eye. It replaces the eye's natural lens that is removed during cataract surgery.
The lens bends (refracts) light rays that enter the eye, helping you to see. Your lens should be clear. But if you have a cataract, your lens has become cloudy. Things look blurry, hazy or less colorful with a cataract. Cataract surgery removes this cloudy lens and replaces it with a clear IOL to improve your vision.
IOLs come in different focusing powers, just like prescription eyeglasses or contact lenses. Your ophthalmologist will measure the length of your eye and the curve of your cornea. These measurements are used to set your IOLs focusing power.
What are IOLs made of?
Most IOLs are made of silicone, acrylic, or other plastic compositions. They are also coated with a special material to help protect your eyes from the sun's harmful ultraviolet (UV) rays.
Monofocal IOLs
The most common type of lens used with cataract surgery is called a monofocal IOL. It has one focusing distance. It is set to focus for up close, medium range or distance vision. Most people have them set for clear distance vision. Then they wear eyeglasses for reading or close work.
Some IOLs have different focusing powers within the same lens. These are called presbyopia-correcting IOLs. These IOLs reduce your dependence on glasses by giving you clear vision for more than one set distance.
Multifocal IOLs
These IOLs provide both distance and near focus at the same time. The lens has different zones set at different powers.
Extended depth-of-focus IOLs:
Similar to multifocal lenses, extended depth-of-focus (EDOF) lenses sharpen near and far vision, but with only one corrective zone, which “extends” to cover both distances. This may mean less effort to re-focus between distances.
Accommodative IOLs
These lenses move or change shape inside your eye, allowing focusing at different distances.
Toric IOLs
For people with astigmatism, there is an IOL called a toric lens. Astigmatism is a refractive error caused by an uneven curve in your cornea or lens. The toric lens is designed to correct that refractive error.
Details
An intraocular lens (IOL) is a lens implanted in the eye usually as part of a treatment for cataracts or for correcting other vision problems such as near-sightedness (myopia) and far-sightedness (hyperopia); a form of refractive surgery. If the natural lens is left in the eye, the IOL is known as phakic, otherwise it is a pseudophakic lens (or false lens). Both kinds of IOLs are designed to provide the same light-focusing function as the natural crystalline lens. This can be an alternative to LASIK, but LASIK is not an alternative to an IOL for treatment of cataracts.
IOLs usually consist of a small plastic lens with plastic side struts, called haptics, to hold the lens in place in the capsular bag inside the eye. IOLs were originally made of a rigid material (PMMA), although this has largely been superseded by the use of flexible materials, such as silicone. Most IOLs fitted today are fixed monofocal lenses matched to distance vision. However, other types are available, such as a multifocal intraocular lens that provides multiple-focused vision at far and reading distance, and adaptive IOLs that provide limited visual accommodation. Multifocal IOLs can also be trifocal IOLs or extended depth of focus (EDOF) lenses.
As of 2021, nearly 28 million cataract procedures took place annually worldwide. That is about 75,000 procedures per day globally. The procedure can be done under local or topical anesthesia with the patient awake throughout the operation. The use of a flexible IOL enables the lens to be rolled for insertion into the capsular bag through a very small incision, thus avoiding the need for stitches. This procedure usually takes less than 30 minutes in the hands of an experienced ophthalmologist, and the recovery period is about two to three weeks. After surgery, patients should avoid strenuous exercise or anything else that significantly increases blood pressure. They should visit their ophthalmologists regularly for three weeks to monitor the implants.
IOL implantation carries several risks associated with eye surgeries, such as infection, loosening of the lens, lens rotation, inflammation, nighttime halos and retinal detachment. Though IOLs enable many patients to have reduced dependence on glasses, most patients still rely on glasses for certain activities, such as reading. These reading glasses may be avoided in some cases if multifocal IOLs, trifocal IOLs or EDOF lenses are used.
Additional Information
IOLs (intraocular lenses) are clear, artificial lenses that replace your eye’s natural ones. You receive IOLs during cataract surgery and refractive lens exchange. IOL implants correct a range of vision issues, including nearsightedness and age-related farsightedness. They may also help reduce your reliance on glasses for certain types of tasks.
What are IOLs?
IOLs (intraocular lenses) are clear artificial lenses that a healthcare provider will implant in your eye to replace your natural lens. Like glasses or contacts, IOL implants can correct vision issues such as:
* Myopia (nearsightedness).
* Hyperopia (farsightedness).
* Presbyopia (age-related farsightedness).
* Astigmatism (altered eye shape).
IOL implants are permanent, meaning they stay in your eyes for the rest of your life. IOLs help improve your vision and may reduce your reliance on glasses in your daily routine. You receive IOLs during eye lens replacement surgery, most commonly during cataract surgery.
Who needs intraocular lens implants?
You may benefit from IOL implants if you:
* Have cataracts that prevent you from seeing clearly. Virtually everyone undergoing cataract surgery will need to have an IOL implant in order to restore vision.
* Have refractive errors that affect your vision, but you’re not a candidate for LASIK or other vision correction surgeries.
What are the different types of intraocular lenses?
There are many types of IOLs, each with its own pros and cons. The main drawback with some types of IOLs is you’ll still need to wear glasses for some tasks (like reading). Some IOLs can reduce your reliance on glasses, but you may notice side effects like glare around lights at night.
The list below covers some general categories of IOLs. Ask your ophthalmologist about which type of IOL is best for you. They’ll help you customize your IOL selection to suit your vision needs, lifestyle and personal preferences.
Monofocal lenses
This is the type of IOL that most people select. Monofocal lenses have one focusing power. This means they sharpen either your distance, mid-range or close-up vision. Most people set their monofocal lenses for distance vision, which can help with tasks like driving. You’ll probably still need glasses for close-up vision.
Monofocal lenses with monovision
Monofocal IOLs set to monovision are a good option for some people who want to rely less on glasses. Normally, the monofocal IOLs for both of your eyes are set to the same range (like distance). But with monovision, the lens for each eye has a different focusing power. For example, the lens for your right eye might correct for distance, with the lens for your left eye correcting for close-up vision.
With monovision, your eyes work together to help you see both distant and close-up objects. One drawback is that it takes some time to adapt to monovision. Some people can’t adapt to monovision at all. So, before choosing monovision IOLs, your provider may suggest you try monovision contact lenses for a couple of weeks. This allows you to see if this method of correction feels comfortable to you.
Multifocal lenses
Multifocal lenses improve your close-up and distance vision and may reduce your need for glasses. Unlike monofocal lenses, multifocal lenses contain several focal zones. Your brain adjusts to these zones and chooses the focusing power you need for any given task (like driving or reading). You may need some time to adapt to these lenses. But over time, you should be able to rely less on your reading glasses. Some people don’t need glasses at all.
One drawback of multifocal lenses is that you may notice rings or halos around lights, like when driving at night.
Extended depth-of-focus (EDOF) lenses
Unlike multifocal lenses, EDOF lenses contain one long focal point that expands your corrected range of vision and depth of focus. These lenses give you excellent distance vision along with improvements in your mid-range vision (for tasks such as computer use). You may still need to use glasses for close-up tasks like reading.
Accommodative lenses
These lenses are similar to your eyes’ natural lenses in that they adjust their shape to help you see close-up or distant objects. Accommodative lenses are another option to help reduce dependency on glasses. But you may prefer to use glasses if you’re reading or focusing on close-up objects for longer periods of time.
Toric lenses
Toric lenses help people who have astigmatism. These lenses improve how light hits your retina, allowing you to have a sharper, clearer vision. Toric lenses are available in monofocal, multifocal, extended depth of focus (EDOF) or accommodative models. They serve to improve the quality of the vision delivered. Toric lenses will help reduce the amount of glare and halos artifacts commonly experienced by people with astigmatism.
Light-adjustable lenses (LALs)
Light-adjustable lenses are different from other IOL options in that your ophthalmologist fine-tunes their corrective power after your lens replacement surgery. They do this through a series of UV light treatment procedures, spaced several days apart. These procedures customize your lens prescription to bring you as close to your desired visual outcome as possible. This is still a type of monofocal lens, so glasses will be necessary for reading or driving.
Phakic lenses
Phakic lenses are typically implanted in younger individuals while trying to preserve the natural human lens, to correct for near-sightedness in people who don’t qualify for laser refractive surgery. This helps preserve your natural ability to focus and accommodate. These lenses will eventually have to be removed during cataract surgery but can offer younger people clear vision for a long time.
Which intraocular lens is best for me?
Your ophthalmologist will determine if you would benefit from cataract surgery, or if you would qualify for a refractive lens exchange surgery. They’ll discuss your options and help you decide which IOLs are best for you. They’ll also conduct a thorough eye exam to check your vision and the health of your eyes. They’ll perform some simple, painless tests to measure your eye size and shape, too.
To prepare for a conversation with your ophthalmologist, you should think about your priorities for your IOLs, as well as aspects that aren’t as important to you. It may help to ask yourself the following questions:
* Am I OK wearing glasses sometimes? If so, how often and for what types of tasks?
* What kind of vision is required in my work/profession? Am I OK wearing glasses for these tasks?
* Do I drive often at night? If so, can I adapt to seeing glare and halos around lights when I drive?
* What kind of hobbies and activities do I enjoy the most and how much dependency on glasses am I OK with for these activities?
* What is my budget for surgery?
Most insurance plans cover monofocal lenses, but you may have to pay for other types out of pocket. Be sure to find out the cost of various IOL options before making your final decision.
What are possible issues and complications related to IOL implantation?
Most IOL complications are rare and include:
* Posterior capsular opacification:This is commonly known as a secondary cataract. This happens after many months or years when a film-like material grows behind the implanted lens. This is a normal process that happens after surgery and can be expected to occur over time for almost everyone. The treatment for this is very quick and straightforward and is usually performed using a laser in the office.
* IOL dislocation: This means your IOL shifts from its normal position. You face a higher risk if you have certain eye conditions, like pseudoexfoliation syndrome, or have had trauma or prior eye surgeries. Certain genetic disorders, such as Ehlers-Danlos syndrome and Marfan syndrome, may also raise your risk. In some cases, you may need surgery to reposition or replace the IOL.
* Uveitis-glaucoma-hyphema (UGH) syndrome: UGH syndrome occurs when an IOL irritates your iris and other parts of your eye. This leads to inflammation, raised intraocular pressure and other symptoms. As with IOL dislocation, you may need surgery to reposition or replace the IOL. This is an extremely rare complication that most people don’t experience with routine surgery.
* IOL opacification: This is a clouding of your IOL. Your vision may become less sharp, and you may notice glare around lights. Treatment involves surgery to give you a new IOL. This is extremely uncommon with modern-day IOLs.
* Refractive surprise: A refractive surprise is when your vision after IOL implantation isn’t as sharp as you and your ophthalmologist expected. Your ophthalmologist will suggest a range of solutions. You may decide to accept the vision correction as is and do nothing further. Or you can choose to wear glasses, have laser vision correction (such as LASIK or PRK) or have an IOL replacement surgery.
Talk with your ophthalmologist about possible complications and your level of risk before choosing to have IOLs implanted in your eyes. They’ll tell you what to expect based on your medical history, eye health and other factors. Also, ask them about common side effects associated with cataract surgery or refractive lens exchange. Be sure to get all the information you need to make the decision that’s right for you.
LASIK
LASIK is a laser eye surgery that corrects vision problems. It changes the shape of your cornea to improve how light hits your retina. This improves your vision. About 99% of people have uncorrected vision that’s 20/40 or better after their LASIK surgery. More than 90% end up with 20/20 vision. Dry eye is the most common side effect.
PRK
Photorefractive keratectomy (PRK) is a laser eye surgery similar to LASIK. Unlike LASIK, which involves opening a flap in your cornea, PRK removes your cornea so that it grows back naturally. That makes it a better laser eye surgery choice for some people who can’t undergo LASIK.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2714 2026-03-06 00:04:02
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2513) Neurotransmitters
Gist
Neurotransmitters are endogenous chemical messengers that transmit signals across a synapse from one neuron to another target cell (neuron, muscle, or gland). They are vital for brain function, influencing mood, sleep, memory, and motor control. Over 50 types exist, acting as either excitatory (triggering a response) or inhibitory (inhibiting a response).
Neurotransmitters are often referred to as the body's chemical messengers. They are the molecules used by the nervous system to transmit messages between neurons, or from neurons to muscles.
Neurotransmitters are endogenous chemical messengers that transmit signals across a synapse between neurons, muscles, or gland cells, essential for regulating body functions, emotions, and thoughts. They are classified into amino acids, peptides, monoamines, purines, and gasotransmitters, with over 50 types known. Their action is either excitatory (promoting a signal) or inhibitory (stopping a signal).
Summary
A neurotransmitter is a signaling molecule secreted by a neuron to affect another cell across a synapse. The cell receiving the signal, or target cell, may be another neuron, but could also be a gland or muscle cell.
Neurotransmitters are released from synaptic vesicles into the synaptic cleft where they are able to interact with neurotransmitter receptors on the target cell. Some neurotransmitters are also stored in large dense core vesicles. The neurotransmitter's effect on the target cell is determined by the receptor it binds to. Many neurotransmitters are synthesized from simple and plentiful precursors such as amino acids, which are readily available and often require a small number of biosynthetic steps for conversion.
Neurotransmitters are essential to the function of complex neural systems. The exact number of unique neurotransmitters in humans is unknown, but more than 100 have been identified. Common neurotransmitters include glutamate, GABA, acetylcholine, glycine, dopamine and norepinephrine.
(GABA: gamma-aminobutyric acid).
Details
Neurotransmitters are your body’s chemical messengers. They carry messages from one nerve cell across a space to the next nerve, muscle or gland cell. These messages help you move your limbs, feel sensations, keep your heart beating, and take in and respond to all information your body receives from other internal parts of your body and your environment.
What are neurotransmitters?
Neurotransmitters are chemical messengers that your body can’t function without. Their job is to carry chemical signals (“messages”) from one neuron (nerve cell) to the next target cell. The next target cell can be another nerve cell, a muscle cell or a gland.
Your body has a vast network of nerves (your nervous system) that send and receive electrical signals from nerve cells and their target cells all over your body. Your nervous system controls everything from your mind to your muscles, as well as organ functions. In other words, nerves are involved in everything you do, think and feel. Your nerve cells send and receive information from all body sources. This constant feedback is essential to your body’s optimal function.
What body functions do nerves and neurotransmitters help control?
Your nervous system controls such functions as your:
* Heartbeat and blood pressure.
* Breathing.
* Muscle movements.
* Thoughts, memory, learning and feelings.
* Sleep, healing and aging.
* Stress response.
* Hormone regulation.
* Digestion, sense of hunger and thirst.
* Senses (response to what you see, hear, feel, touch and taste).
How do neurotransmitters work?
You have billions of nerve cells in your body. Nerve cells are generally made up of three parts:
* A cell body. The cell body is vital to producing neurotransmitters and maintaining the function of the nerve cell.
* An axon. The axon carries the electrical signals along the nerve cell to the axon terminal.
* An axon terminal. This is where the electrical message is changed to a chemical signal using neurotransmitters to communicate with the next group of nerve cells, muscle cells or organs.
Neurotransmitters are located in a part of the neuron called the axon terminal. They’re stored within thin-walled sacs called synaptic vesicles. Each vesicle can contain thousands of neurotransmitter molecules.
As a message or signal travels along a nerve cell, the electrical charge of the signal causes the vesicles of neurotransmitters to fuse with the nerve cell membrane at the very edge of the cell. The neurotransmitters, which now carry the message, are then released from the axon terminal into a fluid-filled space that’s between one nerve cell and the next target cell (another nerve cell, muscle cell or gland).
In this space, called the synaptic junction, the neurotransmitters carry the message across less than 40 nanometers (nm) wide (by comparison, the width of a human hair is about 75,000 nm). Each type of neurotransmitter lands on and binds to a specific receptor on the target cell (like a key that can only fit and work in its partner lock). After binding, the neurotransmitter then triggers a change or action in the target cell, like an electrical signal in another nerve cell, a muscle contraction or the release of hormones from a cell in a gland.
What action or change do neurotransmitters transmit to the target cell?
Neurotransmitters transmit one of three possible actions in their messages, depending on the specific neurotransmitter.
* Excitatory. Excitatory neurotransmitters “excite” the neuron and cause it to “fire off the message,” meaning, the message continues to be passed along to the next cell. Examples of excitatory neurotransmitters include glutamate, epinephrine and norepinephrine.
* Inhibitory. Inhibitory neurotransmitters block or prevent the chemical message from being passed along any farther. Gamma-aminobutyric acid (GABA), glycine and serotonin are examples of inhibitory neurotransmitters.
* Modulatory. Modulatory neurotransmitters influence the effects of other chemical messengers. They “tweak” or adjust how cells communicate at the synapse. They also affect a larger number of neurons at the same time.
What happens to neurotransmitters after they deliver their message?
After neurotransmitters deliver their message, the molecules must be cleared from the synaptic cleft (the space between the nerve cell and the next target cell). They do this in one of three ways.
Neurotransmitters:
* Fade away (a process called diffusion).
* Are reabsorbed and reused by the nerve cell that released it (a process called reuptake).
* Are broken down by enzymes within the synapse so it can’t be recognized or bind to the receptor cell (a process called degradation).
How many different types of neurotransmitters are there?
Scientists know of at least 100 neurotransmitters and suspect there are many others that have yet to be discovered. They can be grouped into types based on their chemical nature. Some of the better-known categories and neurotransmitter examples and their functions include the following:
Amino acids neurotransmitters
These neurotransmitters are involved in most functions of your nervous system.
* Glutamate. This is the most common excitatory neurotransmitter of your nervous system. It’s the most abundant neurotransmitter in your brain. It plays a key role in cognitive functions like thinking, learning and memory. Imbalances in glutamate levels are associated with Alzheimer’s disease, dementia, Parkinson’s disease and seizures.
* Gamma-aminobutryic acid (GABA). GABA is the most common inhibitory neurotransmitter of your nervous system, particularly in your brain. It regulates brain activity to prevent problems in the areas of anxiety, irritability, concentration, sleep, seizures and depression.
* Glycine. Glycine is the most common inhibitory neurotransmitter in your spinal cord. Glycine is involved in controlling hearing processing, pain transmission and metabolism.
Monoamines neurotransmitters
These neurotransmitters play a lot of different roles in your nervous system and especially in your brain. Monoamines neurotransmitters regulate consciousness, cognition, attention and emotion. Many disorders of your nervous system involve abnormalities of monoamine neurotransmitters, and many drugs that people commonly take affect these neurotransmitters.
* Serotonin. Serotonin is an inhibitory neurotransmitter. Serotonin helps regulate mood, sleep patterns, sexuality, anxiety, appetite and pain. Diseases associated with serotonin imbalance include seasonal affective disorder, anxiety, depression, fibromyalgia and chronic pain. Medications that regulate serotonin and treat these disorders include selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs).
* Histamine. Histamine regulates body functions including wakefulness, feeding behavior and motivation. Histamine plays a role in asthma, bronchospasm, mucosal edema and multiple sclerosis.
* Dopamine. Dopamine plays a role in your body’s reward system, which includes feeling pleasure, achieving heightened arousal and learning. Dopamine also helps with focus, concentration, memory, sleep, mood and motivation. Diseases associated with dysfunctions of the dopamine system include Parkinson’s disease, schizophrenia, bipolar disease, restless legs syndrome and attention deficit hyperactivity disorder (ADHD). Many highly addictive drugs (cocaine, methamphetamines, amphetamines) act directly on the dopamine system.
* Epinephrine. Epinephrine (also called adrenaline) and norepinephrine (see below) are responsible for your body’s so-called “fight-or-flight response” to fear and stress. These neurotransmitters stimulate your body’s response by increasing your heart rate, breathing, blood pressure, blood sugar and blood flow to your muscles, as well as heighten attention and focus to allow you to act or react to different stressors. Too much epinephrine can lead to high blood pressure, diabetes, heart disease and other health problems. As a drug, epinephrine is used to treat anaphylaxis, asthma attacks, cardiac arrest and severe infections.
* Norepinephrine. Norepinephrine (also called noradrenaline) increases blood pressure and heart rate. It’s most widely known for its effects on alertness, arousal, decision-making, attention and focus. Many medications (stimulants and depression medications) aim to increase norepinephrine levels to improve focus or concentration to treat ADHD or to modulate norepinephrine to improve depression symptoms.
Peptide neurotransmitters
Peptides are polymers or chains of amino acids.
* Endorphins. Endorphins are your body’s natural pain reliever. They play a role in our perception of pain. Release of endorphins reduces pain, as well as causes “feel good” feelings. Low levels of endorphins may play a role in fibromyalgia and some types of headaches.
Acetylcholine
This excitatory neurotransmitter does a number of functions in your central nervous system (CNS [brain and spinal cord]) and in your peripheral nervous system (nerves that branch from the CNS). Acetylcholine is released by most neurons in your autonomic nervous system regulating heart rate, blood pressure and gut motility. Acetylcholine plays a role in muscle contractions, memory, motivation, sexual desire, sleep and learning. Imbalances in acetylcholine levels are linked with health issues, including Alzheimer’s disease, seizures and muscle spasms.
Why would a neurotransmitter not work as it should?
Several things can go haywire and lead to neurotransmitters not working as they should. In general, some of these problems include:
* Too much or not enough of one or more neurotransmitters are produced or released.
* The receptor on the receiver cell (the nerve, muscle or gland) isn’t working properly. The otherwise normal functioning neurotransmitter can’t effectively signal the next cell.
* The cell receptors aren’t taking up enough neurotransmitter due to inflammation and damage of the synaptic cleft.
* Neurotransmitters are reabsorbed too quickly.
* Enzymes limit the number of neurotransmitters from reaching their target cell.
Problems with other parts of nerves, existing diseases or medications you may be taking can affect neurotransmitters. Also, when neurotransmitters don’t function as they should, disease can happen. For example:
* Not enough acetylcholine can lead to the loss of memory that’s seen in Alzheimer’s disease.
* Too much serotonin is possibly associated with autism spectrum disorders.
* An increase in activity of glutamate or reduced activity of GABA can result in sudden, high-frequency firing of local neurons in your brain, which can cause seizures.
* Too much norepinephrine and dopamine activity and abnormal glutamate transmission contribute to mania.
How do medications affect the action of neurotransmitters?
Scientists recognized the value and the role of neurotransmitters in your nervous system and the importance of developing medications that could influence these chemical messengers to treat many health conditions. Many medications, especially those that treat diseases of your brain, work in many ways to affect neurotransmitters.
Medications can block the enzyme that breaks down a neurotransmitter so that more of it reaches nerve receptors.
Example: Donepezil, galantamine and rivastigmine block the enzyme acetylcholinesterase, which breaks down the neurotransmitter acetylcholine. These medications are used to stabilize and improve memory and cognitive function in people with Alzheimer’s disease, as well as other neurodegenerative disorders.
Medications can block the neurotransmitter from being received at its receptor site.
Example: Selective serotonin reuptake inhibitors are a type of drug class that blocks serotonin from being received and absorbed by a nerve cell. These drugs may be helpful in treating depression, anxiety and other mental health conditions.
Medications can block the release of a neurotransmitter from a nerve cell.
Example: Lithium works as a treatment for mania partially by blocking norepinephrine release and is used in the treatment of bipolar disorder.
Additional Information
Neurotransmitters are chemical messengers in the body. Their function is to transmit signals from nerve cells to target cells. These signals help regulate bodily functions ranging from heart rate to appetite.
Neurotransmitters are part of the nervous system. They play a crucial role in human development and many bodily functions.
What is a neurotransmitter?
The nervous system controls the body’s organs and plays a role in nearly all bodily functions. Nerve cells, also known as neurons, and their neurotransmitters play important roles in this system.
Nerve cells fire nerve impulses. They do this by releasing neurotransmitters, also known as the body’s chemical messengers. These chemicals carry signals to other cells.
Neurotransmitters relay their messages by traveling between cells and attaching to specific receptors on target cells.
Each neurotransmitter attaches to a different receptor. For example, dopamine molecules attach to dopamine receptors. When they attach, it triggers an action in the target cells.
After neurotransmitters deliver their messages, the body breaks them down or recycles them.
What do neurotransmitters do?
The brain needs neurotransmitters to regulate many necessary functions, including:
* heart rate
* breathing
* sleep cycles
* digestion
* mood
* concentration
* appetite
* muscle movement
Neurotransmitters also play a role in early human development.
Types of neurotransmitters
Experts have identified over 100 neurotransmitters to date and are still discovering more.
Neurotransmitters have different types of actions:
* Excitatory neurotransmitters encourage a target cell to take action.
* Inhibitory neurotransmitters decrease the chances of the target cell taking action. In some cases, these neurotransmitters have a relaxation-like effect.
* Modulatory neurotransmitters can send messages to many neurons at the same time. They also communicate with other neurotransmitters.
Some neurotransmitters can carry out several functions depending on the type of receptor they connect to.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2715 2026-03-07 00:03:52
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2514) Arctic Wolf
Gist:
Do Arctic wolves still exist?
They were listed as vulnerable from 1982 to 1995, but their status was upgraded to least concern in 1996 and has remained the same ever since. Thanks to their remote, icy habitat, Arctic wolves live far away from any human populations.
Are Arctic wolves friendly to humans?
The Arctic wolf is relatively unafraid of people, and can be coaxed to approach people in some areas.
Summary
The Arctic fox (Vulpes lagopus), also known as the white fox, polar fox, or snow fox, is a small species of fox native to the Arctic regions of the Northern Hemisphere and common throughout the Arctic tundra. It is well adapted to living in cold environments, and is known for its thick, warm fur that can be used as camouflage against snow in the winter. It has a large and fluffy tail. In the wild, most individuals do not live past their first year but some exceptional ones survive up to 11 years. Its body length ranges from 46 to 68 cm (18 to 27 in), with a generally rounded body shape to minimize the escape of body heat.
The Arctic fox preys on many small creatures such as lemmings, voles, ringed seal pups, fish, waterfowl, and seabirds. It also eats carrion, berries, seaweed, and insects and other small invertebrates. Arctic foxes form monogamous pairs during the breeding season and they stay together to raise their young in complex underground dens. Occasionally, other family members may assist in raising their young. Natural predators of the Arctic fox include golden eagles, Arctic wolves, polar bears, wolverines, red foxes, and brown bears.
Details
The Arctic wolf (Canis lupus arctos), also known as the white wolf, polar wolf, and the Arctic grey wolf, is a subspecies of grey wolf native to the High Arctic tundra of Canada's Queen Elizabeth Islands, from Melville Island to Ellesmere Island. Unlike some populations that move between tundra and forest regions, Arctic wolves spend their entire lives north of the northern treeline. Their southward distribution is limited to the northern fringes of the Middle Arctic tundra on the southern half of Prince of Wales and Somerset Islands.
It is a medium-sized subspecies, distinguished from the northwestern wolf by its smaller size, whiter colouration, narrower braincase, and larger carnassials. Since 1930, there has been a progressive reduction in size in Arctic wolf skulls, which is likely the result of wolf-dog hybridization.
Taxonomy
In 1935, the British zoologist Reginald Pocock attributed the subspecies name Canis lupus arctos (Arctic wolf) to a specimen from Melville Island in the Queen Elizabeth Islands, Canada. He wrote that similar wolves could be found on Ellesmere Island. He also attributed the name Canis lupus orion to a Greenland wolf specimen from Cape York, northwest Greenland. Both wolves are recognized as separate subspecies of Canis lupus in the taxonomic authority Mammal Species of the World (2005).
A study by Chambers et al. (2012) using autosomal microsatellite DNA and Mitochondrial DNA data indicate that the Arctic wolf has no unique haplotypes which suggests that its colonization of the Arctic Archipelago from the North American mainland was relatively recent, and thus not sufficient to warrant subspecies status. During a meeting assembled in 2014 by the National Center for Ecological Analysis and Synthesis of the United States Fish and Wildlife Service, one speaker, Robert K. Wayne, mentioned he disagreed with the conclusion that a subspecies had to be genetically distinct, believing that different subspecies could slowly grade into each other - suggesting that although it was impossible to determine if an individual wolf was one subspecies or the next using DNA, the population of Arctic wolves as a whole could be distinguished by the looking at the proportions of single-nucleotide polymorphisms (SNP): i.e. Arctic wolves could be distinguished by having three wolves in the putative population with a specific SNP, whereas another subspecies could be distinguished by having 20 wolves with that SNP. Wayne furthermore stated that he believed the habitat in which the wolf happened to be found was a good enough characteristic to distinguish a subspecies.
Behaviour
The Arctic wolf is relatively unafraid of people, and can be coaxed to approach people in some areas. The wolves on Ellesmere Island do not fear humans, which is thought to be due to them seeing humans so little, and they will approach humans cautiously and curiously. Otto Sverdrup wrote that during the Fram expedition, a pair of wolves shadowed one of his teammates, who kept them at a distance by waving his ski pole. In 1977, a pair of scientists were approached by six wolves on Ellesmere Island, with one animal leaping at one of the scientists and grazing a cheek. A number of incidents involving aggressive wolves have occurred in Alert, Nunavut, where the wolves have lived in close proximity to the local weather station for decades and became habituated to humans. One of these wolves attacked 3 people, was shot, and tested positive for rabies.
Very little is known about the movement of the Arctic wolves, mainly due to climate. The only time at which the wolf migrates is during the wintertime when there is complete darkness for 24 hours. This makes Arctic wolf movement hard to research. About 2,250 km (1,400 mi) south of the High Arctic, a wolf movement study took place in the wintertime in complete darkness, when the temperature was as low as −53 °C (−63 °F). The researchers found that wolves prey mainly on the muskoxen. There is no available information of the wolves' movements where the muskoxen were.
Diet
In the wild, Arctic wolves primarily prey on muskoxen and Arctic hares. They have also been found to prey on lemmings, caribou, Arctic foxes, birds, and beetles. It has been also found that Arctic wolves scavenge through garbage. This sort of food source will not always be found in the Arctic wolf's diet because of regional and seasonal availability. There is some debate whether the muskox or the Arctic hare is the primary prey for the hare-wolf-muskox predator-prey system. Evidence suggests that muskoxen provide long-term viability and other ungulates do not appear in the wolf's diet. Evidence suggesting that Arctic wolves depend more on hares claims that the mature wolf population paralleled the increase of hares rather than muskoxen availability. However, the degree of reliance between the two sources of food is uncertain and the amount of consumption between the two species also depends on the season and year. Debate continues when seasonal variations and the diet of young wolves is discussed. According to one study, muskox calves serve as a primary food source because the needs of pups are greater but another study suggests that "when hares were much more plentiful (Mech, 2000), wolves commonly fed them to their pups during summer." These differences may be attributed to location as well. Polar bears are rarely encountered by wolves, though there are two records of wolf packs killing polar bear cubs.
Conservation
The Arctic wolf is least concern, but it does face threats. In 1997, there was a decline in the Arctic wolf population and its prey, muskoxen (Ovibos moschatus), and Arctic hares (Lepus arcticus). This was due to unfavourable weather conditions during the summers for four years. Arctic wolf populations recovered the next summer when weather conditions returned to normal.
Additional Information
Arctic wolves have white fur year-round which allows them to blend into their snowy surroundings. Their coat is long and silky with soft, thick under fur. This is shed in the spring and the coat becomes shorter and less dense. The lengthy tail is bushy, and the legs are long giving it a lanky appearance. The feet are large and digitate with non-retractable claws. The forefeet have five toes and the hind feet have four. The skull is broad and the face and ears are well defined. Ears are slightly rounded and the face is less pointed than other species of wolf. This wolf is a subspecies of the gray wolf (Canis lupus). The year-round white coats and slightly shorter ears and noses distinguish them from the other subspecies of Canis lupus. They are also slightly smaller in stature. Male Arctic wolves generally weigh between 34 – 46 kg, and females between 36 – 38 kg.
Distribution
This sub-species lives primarily in the Arctic, the region located above 67 degrees north latitude. This is the area along the northern edge of the North American continent and northward to the North Pole, as well as along the eastern and northern shores of Greenland.
Habitat
The land in the Arctic is covered with snow and ice for most of the year except for brief periods during the summer months. Due to scarcity of grazing plants and resulting low density of prey species, wolves roam over large areas hunting for food.
Diet
They are predatory carnivores. They hunt in packs for caribou and musk-oxen. They also consume Arctic hares, ptarmigan, lemmings, and other small animals including nesting birds.
Reproduction
These wolves live in groups of seven to ten individuals. There is a highly complex social order within wolf packs and each pack has a dominant male and female, who bond for life. Mating between the pair takes place during the breeding season of January through to March. The gestation period for the pregnant alpha female is from 53 to 61 days. Permafrost in the Arctic makes it difficult for the wolves to dig dens. Instead, their dens are often rock outcroppings, caves, or shallow depressions in the tundra soil. The mother gives birth to two or three pups in late May to early June. Litter size is smaller for Arctic wolves. Pups are born blind and deaf. They have soft, fuzzy dark hair with small, droopy ears and blunt muzzles. They are entirely dependent on their mother; she is the only one who has contact with them at this time. She in turn relies on her mate to bring her food. At about ten days the pups’ eyes open and at three weeks they can hear. After a month the pups are able to eat meat. From then on the whole pack shares the job of feeding them, bringing meat which they regurgitate for the pups. Each member of the pack will affectionately lick, nuzzle, and sniff each pup. They become caregivers - providing food, play, and protection. Pups respond with squeaks and tail wags. They nibble and lick the feeder’s muzzle to stimulate regurgitation. They leave the den after eight to ten weeks to discover the outside world. As pups they are already establishing, through play, their future roles within the pack. When the pack hunts, one adult member will remain as a puppy sitter. Pups have grown strong enough to travel at six months of age, and from that time will join the other members of the pack learning survival skills. They become sexually mature at two to three years of age.
Adaptation
Wolves communicate with each other in a variety of ways. Clear communication is a key element to the success of a cooperative pack.
Body language: They have a rich vocabulary of visual signs that communicate social rank, mood, and intentions. Subtle changes in tail and ear positions, of body and head angle, making and breaking eye contact, and facial expressions are just a few. Tail movements for example are related to various feelings: friendliness, aggression, fear, status, social tension, threat, and submission are all communicated via tail position.
Vocalization: Wolves howl for many reasons, to assemble the pack before and after hunts, to locate members of the pack over distances, to warn neighboring packs of their presence, and apparently just for the fun of it. They often howl at a rendezvous site. The wolf’s howl can be heard up to 5 km away. They also growl, snarl, whine, yip, whimper, and bark.
Signs: They use scent marking to communicate their presence and territory boundaries to other wolves. This can be either urine or feces left on rocks and snow banks along their hunting trails. Wolves have a very good sense of smell. They can detect prey 1.6 km away and can sense an animal three days after it has gone.
Wolves are very social animals and live in family packs for protection and for hunting.
Pack structure: There is an alpha pair in each pack. The alpha male is the leader. Only the alpha couple breeds and with only one litter per pack. The number of pups is low in relationship to the number of adults. Wolves have concern for other wolves in the pack, with the younger members feeding and protecting the older wolves. All adults co-operate in feeding and educating the young. Wolf pack members protect each other.
Hunting: Life in a pack is extremely important to the survival of Arctic wolves. They live in very harsh conditions. Hunting together allows them to kill larger prey including musk oxen and caribou. A successful hunt depends on the cooperative efforts of the entire pack.
Wolves demonstrate intelligence in choosing prey: they look for old, sick, or weak animals that are easier to catch. Wolves work hard for their prey; they kill only one of every ten large mammals they chase. They eat all of the catch, including the bones. They have 42 teeth. Four large canine teeth are used for hanging onto and biting through flesh. Molars at the back are specialized shearing teeth referred to as carnassials. When hunting alone a wolf catches smaller animals.
Arctic wolves are well adapted to icy conditions. White fur allows them to blend into snowy surroundings. To help reduce heat loss their ears are small and rounded, the muzzle is short, and the fur is dense. Legs are shorter than other subspecies. They have tufts of hair between the pads of their feet.
Threats to Survival
Polar bears sometimes prey on Arctic wolves. Global climate change may affect these wolves. Exploration of the natural resources such as oil and gas will no doubt have an impact.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2716 2026-03-08 00:08:41
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2515) Baltic States
Gist
The Baltic states—Estonia, Latvia, and Lithuania—are three sovereign nations in Northern Europe on the eastern coast of the Baltic Sea. Gaining independence from the Soviet Union in 1991, they are now parliamentary republics, members of the EU, NATO, and the OECD, featuring high-income economies, high living standards, and a shared history.
The Baltic States receive their name from the Baltic Sea, which borders them. Lithuania, Estonia, and Latvia are bounded on the west and north by the Baltic Sea.
Summary
The Baltic states[a] or the Baltic countries is a geopolitical term encompassing Estonia, Latvia, and Lithuania. All three countries are members of NATO, the European Union, the Eurozone, and the OECD. The three sovereign states on the eastern coast of the Baltic Sea are sometimes referred to as the "Baltic nations", less often and in historical circumstances also as the "Baltic republics", the "Baltic lands", or simply the Baltics.
All three Baltic countries are classified as high-income economies by the World Bank and maintain a very high Human Development Index. The three governments engage in intergovernmental and parliamentary cooperation. There is also frequent cooperation in foreign and security policy, defence, energy, and transportation.
NATO: North Atlantic Treaty Organization.
OECD: Organisation for Economic Co-operation and Development.
Geography
The Baltic States cover an area of 175,228 square kilometres (67,656 sq mi) (roughly twice the size of mainland Portugal), with a population of 6,132,500 (2024). Bordered by the Baltic Sea to the west and the north, they share borders with Russia, Belarus, and Poland. The Kaliningrad Oblast, formerly known as Königsberg in Germany, is landlocked between Lithuania and Poland and belongs to Russia.
The terrain of this region is relatively flat, punctuated by numerous lakes and ponds, particularly in the north, and hills in Lithuania.
General statistics
All three are unitary republics, which simultaneously joined the European Union on 1 May 2004, share EET/EEST time zone schedules and the euro currency.
EET: Eastern European Time.
EEST: Eastern European Summer Time.
Details
Baltic states are the northeastern region of Europe containing the countries of Estonia, Latvia, and Lithuania, on the eastern shores of the Baltic Sea.
The Baltic states are bounded on the west and north by the Baltic Sea, which gives the region its name, on the east by Russia, on the southeast by Belarus, and on the southwest by Poland and an exclave of Russia. The underlying geology is sandstone, shale, and limestone, evidenced by hilly uplands that alternate with low-lying plains and bear mute testimony to the impact of the glacial era. In fact, glacial deposits in the form of eskers, moraines, and drumlins occur in profusion and tend to disrupt the drainage pattern, which results in frequent flooding. The Baltic region is dotted with more than 7,000 lakes and countless peat bogs, swamps, and marshes. A multitude of rivers, notably the Neman (Lithuanian: Nemunas) and Western Dvina (Latvian: Daugava), empty northwestward into the Baltic Sea.
The climate is cool and damp, with greater rainfall in the interior uplands than along the coast. Temperatures are moderate in comparison with other areas of the East European Plain, such as in neighbouring Russia. Despite its extensive agriculture, the Baltic region remains more than one-third forested. Trees that adapt to the often poorly drained soil are common, such as birches and conifers. Among the animals that inhabit the region are elk, boar, roe deer, wolves, hares, and badgers.
The Latvian and Lithuanian peoples speak languages belonging to the Baltic branch of the Indo-European linguistic family and are commonly known as Balts. The Estonian (and Livonian) peoples, who are considered Finnic peoples, speak languages of the Finno-Ugric family and constitute the core of the southern branch of the Baltic Finns. Culturally, the Estonians were strongly influenced by the Germans, and traces of the original Finnish culture have been preserved only in folklore. The Latvians also were considerably Germanized, and the majority of both the Estonians and the Latvians belong to the Lutheran church. However, most Lithuanians, associated historically with Poland, are Roman Catholic.
The vast majority of ethnic Estonians, Latvians, and Lithuanians live within the borders of their respective states. In all three countries virtually everyone among the titular nationalities speaks the native tongue as their first language, which is remarkable in light of the massive Russian immigration to the Baltic states during the second half of the 20th century. Initially, attempts to Russify the Baltic peoples were overt, but later they were moderated as Russian immigration soared and the sheer weight of the immigrant numbers simply served to promote this objective in less-blatant ways. Independence from the Soviet Union in 1991 allowed the Baltic states to place controls on immigration, and, in the decade following, the Russian presence in Baltic life diminished. At the beginning of the 21st century, the titular nationalities of Lithuania and Estonia accounted for about four-fifths and two-thirds of the countries’ populations, respectively, while ethnic Latvians made up just less than three-fifths of their nation’s population. Around this time, Poles eclipsed Russians as the largest minority in Lithuania. Urban dwellers constitute more than two-thirds of the region’s population, with the largest cities being Vilnius and Kaunas in southeastern Lithuania, the Latvian capital of Riga, and Tallinn on the northwestern coast of Estonia. Life expectancy in the Baltic states is comparatively low by European standards, as are the rates of natural increase, which were negative in all three countries at the beginning of the 21st century, owing in part to an aging population. Overall population fell in each of the Baltic states in the years following independence, primarily because of the return emigration of Russians to Russia, as well as other out-migration to western Europe and North America. In some cases, Russians took on the nationalities of their adopted Baltic countries and were thus counted among the ethnic majorities.
After the breakup of the Soviet Union, the Baltic states struggled to make a transition to a market economy from the system of Soviet national planning that had been in place since the end of World War II. A highly productive region for the former U.S.S.R., the Baltic states catered to economies of scale in output and regional specialization in industry—for example, manufacturing electric motors, machine tools, and radio receivers. Latvia, for example, was a leading producer of Soviet radio receivers. Throughout the 1990s privatization accelerated, national currencies were reintroduced, and non-Russian foreign investment increased.
Agriculture remains important to the Baltic economy, with potatoes, cereal grains, and fodder crops produced and dairy cattle and pigs raised. Timbering and fisheries enjoy modest success. The Baltic region is not rich in natural resources. Though Estonia is an important producer of oil shale, a large share of mineral and energy resources is imported. Low energy supplies, inflationary prices, and an economic collapse in Russia contributed to an energy crisis in the Baltics in the 1990s. Industry in the Baltic states is prominent, especially the production of food and beverages, textiles, wood products, and electronics and the traditional stalwarts of machine building and metal fabricating. The three states have the highest productivity of the former constituent republics of the Soviet Union.
Shortly after attaining independence, Estonia, Latvia, and Lithuania abandoned the Russian ruble in favour of new domestic currencies (the kroon, lats, and litas, respectively), which, as they strengthened, greatly improved foreign trade. The main trading partners outside the region are Russia, Germany, Finland, and Sweden. The financial stability of the Baltic nations was an important prerequisite to their entering the European Union and the North Atlantic Treaty Organization in 2004. Estonia, Latvia, and Lithuania each adopted the euro as its common currency in 2011, 2014, and 2015, respectively.
This article covers the history of the region from antiquity to the post-Soviet period. Additional information on the region’s physical and human geography can be found in the article Europe. Area 67,612 square miles (175,116 square km). Pop. (2020 est.) 5,841,000.
Additional Information:
What are the Baltic States?
The term Baltic States refers to a group of independent countries that border the Baltic Sea. The Baltic States are composed of three countries: Lithuania, Estonia, and Latvia. Combined, the countries are no more significant in size than the state of Missouri.
The Baltic States or Baltic countries are located in the northeastern region of Europe. These countries gained independence from the Russian Empire in the 1910s and regained independence from the Soviet Union in the 1990s.
While the population of the Baltic states is quite small, each country has a major city as its capital: Tallinn in Estonia; Rīga in Latvia; and Vilnius in Lithuania. Each city has an old town, with historic buildings reflecting their German heritage. Rīga also has a large number of art nouveau buildings. The legacy of the Soviet Union is gradually being erased, although many Soviet-era apartment blocks remain. The capital cities are the seat of government, with many administrative offices in them. Economic activity is intense: Rīga and Tallinn are both important port cities, while Vilnius has emerged as a major financial center. In recent years, the Baltic capitals have become tourist destinations as foreigners have come to appreciate their attractions.
Song Traditions
One of the most significant cultural traditions in the Baltic states is the singing of folk songs, of which there are thousands. Traditional dance is also important. Children begin to learn singing and dance at an early age, often becoming part of ensembles that perform publicly. Mass song and dance festivals, involving tens of thousands of people, are held on a regular basis, with a great deal of audience participation. The importance of these festivals has been officially recognized by UNESCO, which declared them to be Masterpieces of the Oral and Intangible Heritage of Humanity. This year, many festivities, including folk singing and dancing, will be held in all three Baltic states as part of the celebration of the 100th anniversary of independence for Estonia, Latvia, and Lithuania. The tradition of song and dance festivals has been maintained by Baltic communities in the United States, Canada, and elsewhere.
Celebrating Nature
A reverence for nature has always been at the heart of traditional Baltic culture, and it continues in the present day. The celebration of the mid-summer solstice is one of the most important holidays on the calendar, and all three countries basically shut down for two days. People go to the countryside, where they build bonfires and sing songs until late in the night. The natural splendor of the Baltic countries was endangered by pollution and development in the Soviet period, but now environmental protection is a high priority. The region’s natural beauty is a primary attraction for visitors from all over the world.
Innovation and Development
The traditional economies of the Baltic countries were based on timber, dairy products, and agriculture. These all remain important, but after the end of the Soviet period, Estonia, Latvia, and Lithuania have undergone a major economic transformation as new sectors have been developed in the areas of computer software, electronics, and ICT (Information and Communications Technology) products. Of the three Baltic states, Estonia has taken the lead in this process, with its development of commercial services such as Skype and governmental programs related to building e-society infrastructure. Latvia and Lithuania have also invested heavily in the electronics sphere. All three Baltic countries have developed close connections with Silicon Valley, with many Baltic companies basing their operations here. It is likely that e-commerce will continue to grow in the Baltic states as their highly educated professional classes make more innovations.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2717 2026-03-09 00:03:28
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2516) Sodium Phosphate
Gist
Sodium phosphate is a versatile salt (H3PO4) used as a food additive (emulsifier, buffer, leavening agent), cleaning agent, and saline laxative for colonoscopies. It exists in mono-, di-, and tribasic forms, often used in processed foods and medical treatments. While generally safe, excessive consumption can cause serious side effects.
Consuming small amounts of foods that contain sodium phosphate is "most likely" not harmful to your health. However, since many people consume fast food, processed meats and packaged foods on a daily basis, there is concern that high levels of sodium phosphate can harm the body.
Summary
A sodium phosphate is a generic variety of salts of sodium (Na+) and phosphate. Phosphate also forms families or condensed anions including di-, tri-, tetra-, and polyphosphates. Most of these salts are known in both anhydrous (water-free) and hydrated forms. The hydrates are more common than the anhydrous forms.
Uses
Sodium phosphates have many applications in food and for water treatment. Sodium phosphates are often used as water-retaining agents for frozen food, thickening agents for processed food, and leavening agents for baked goods. It is also a source of the phosphate ion (an emulsifying agent) for processed cheese, where it chelates calcium, thereby allowing the casein in cheese to remain suspended and preventing separation during heating. They are also used to control pH of processed foods.
They are also used in medicine for constipation and to prepare the bowel for medical procedures, by acting as an osmotic laxative that draws water into the bowel.
Like other phosphate salts they are used in detergents to increase their activity in hard water. They are also used in water softeners in addition to regular sodium chloride.
They are also useful corrosion inhibitors for preventing rusting of metal pipes.
Adverse effects
Sodium phosphates are popular in commerce in part because they are inexpensive and because they are nontoxic at normal levels of consumption. However, oral sodium phosphates when taken at high doses for bowel preparation for colonoscopy may in some individuals carry a risk of kidney injury under the form of phosphate nephropathy. There are several oral phosphate formulations which are prepared extemporaneously. Oral phosphate prep drugs have been withdrawn in the United States, although evidence of causality is equivocal. Since safe and effective replacements for phosphate purgatives are available, several medical authorities have recommended general disuse of oral phosphates.
Details:
Description
Sodium phosphate is a colorless to white crystalline powder or granules. It is prepared by neutralization of phosphoric acid under controlled conditions with sodium hydroxide or sodium carbonate .
We are committed to bringing you Greener Alternative Products, which belong to one of the four categories of greener alternatives. Sodium phosphate supports cleaner technologies as a versatile buffering and stabilizing agent that helps control pH, mitigate corrosion and side reactions, and extend equipment/component lifetimes—reducing waste, chemical use, and energy demand across processes.
Application
Sodium phosphate is used as a:
* component in the preparation of solid crystals of calcium hydroxyapatite substituted by strontium
* block buffer to study segmental and subcellular distribution of CFTR in the kidney
(CFTR: The Cystic Fibrosis Transmembrane Conductance Regulator is a protein-coding gene and ion channel that transports chloride and bicarbonate ions across epithelial cell membranes, crucial for regulating fluid balance in the lungs and pancreas. Mutations in the CFTR gene cause cystic fibrosis, leading to thick, sticky mucus, chronic infections, and organ damage.)
Additional Information:
What is Sodium Phosphate?
Sodium phosphate also known as phospho soda with the formula Na3PO4 is a saline cathartic that is familiar to radiologists since it is often used as a cleansing agent prior to double contrast barium enema.
It is prepared by neutralization of phosphoric acid under controlled conditions with sodium hydroxide or sodium carbonate. Sodium phosphate cradles are the most widely recognized, yet there is broad utilization of potassium phosphate buffer and blends of sodium and potassium. Many compounds of pharmaceutical interest are formulated in sodium phosphate buffers.
Uses of Sodium Phosphate – Na3PO4
* Short-term, local treatment of inflammation with neomycin as bacterial prophylaxis.
* Used after glaucoma surgery or after cataract surgery.
* Used as a mild laxative, stimulates the emptying of the gall bladder.
* One of the most palatable of the saline laxatives. It is also used in the form of an oral solution as an antihypercalcemia.
* Used to control the pH of water hardness precipitation and control agent in mildly acidic solutions.
Frequently Asked Questions
Q1. Is sodium phosphate an acid or a base?
A1. Sodium phosphate is a salt obtained by the reaction of phosphoric acid and sodium hydroxide.
Q2. What is sodium phosphate used for in medicine?
A2. Sodium biphosphate and sodium phosphate are sources of phosphorus which is a material that occurs naturally and is essential in every cell in the body. Sodium biphosphate and sodium phosphate is a combination drug used in adults before a colonoscopy to relieve constipation and cleanse the intestines.
Q3. What happens if your phosphate levels are low?
A3. High phosphate levels seldom contribute to hypophosphatemia symptoms; rather symptoms generally arise from the underlying disorder that causes hypophosphatemia. Ultra low levels of phosphate can cause difficulty breathing, agitation, altered mental state, muscle weakness and muscle damage called rhabdomyolysis.
Q4. What is sodium phosphate monobasic monohydrate?
A4. Sodium Phosphate, monobasic (monohydrate) is a reagent commonly used in molecular biology, biochemistry, and chromatography with a very high buffering capacity. Monobasic sodium phosphate is extremely hygroscopic and soluble in water.
Q5. What is the difference between sodium phosphate monobasic and dibasic?
A5. Sodium phosphate monobasic has the chemical formula of NaH2PO4, and the chemical formula of Na2HPO4 has sodium phosphate dibasic. As sodium phosphate dibasic dissolves in water, the basicity in the medium is higher than when monobasic sodium phosphate dissolves in water.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2718 2026-03-10 00:04:55
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2517) Hyperglycemia
Gist
Hyperglycemia is high blood sugar, commonly affecting diabetics when glucose exceeds 125 mg/dL (fasting) or 180 mg/dL (postprandial) due to low insulin, skipped medication, or stress. Symptoms include increased thirst, frequent urination, fatigue, and blurred vision. Long-term effects include severe nerve, kidney, heart, and eye damage.
Hyperglycemia treatment focuses on lifestyle changes (diet, exercise, hydration), monitoring blood sugar, and taking prescribed medications like insulin or oral agents (e.g., metformin), with emergency care for severe cases like Diabetic Ketoacidosis (DKA) involving IV fluids and insulin, aiming to prevent long-term complications like kidney or eye disease.
Summary
Hyperglycemia is an unusually high amount of glucose in the blood. It is defined as blood glucose level exceeding 6.9 mmol/L (125 mg/dL) after fasting for 8 hours or 10 mmol/L (180 mg/dL) 2 hours after eating.
Signs and symptoms
Hyperglycemia may be asymptomatic. Blood glucose levels can rise above normal and cause pathological and functional changes for significant periods without producing any permanent effects or symptoms. During this asymptomatic period, an abnormality in carbohydrate metabolism can occur, which can be tested by measuring plasma glucose.
The degree of hyperglycemia can change over time depending on the metabolic cause, for example, impaired glucose tolerance or fasting glucose, and it can depend on treatment.
Details:
Overview
High blood sugar, also called hyperglycemia, affects people who have diabetes. Several factors can play a role in hyperglycemia in people with diabetes. They include food and physical activity, illness, and medications not related to diabetes. Skipping doses or not taking enough insulin or other medication to lower blood sugar also can lead to hyperglycemia.
It's important to treat hyperglycemia. If it's not treated, hyperglycemia can become severe and cause serious health problems that require emergency care, including a diabetic coma. Hyperglycemia that lasts, even if it's not severe, can lead to health problems that affect the eyes, kidneys, nerves and heart.
Symptoms
Hyperglycemia usually doesn't cause symptoms until blood sugar (glucose) levels are high — above 180 to 200 milligrams per deciliter (mg/dL), or 10 to 11.1 millimoles per liter (mmol/L).
Symptoms of hyperglycemia develop slowly over several days or weeks. The longer blood sugar levels stay high, the more serious symptoms may become. But some people who've had type 2 diabetes for a long time may not show any symptoms despite high blood sugar levels.
Early signs and symptoms
Recognizing early symptoms of hyperglycemia can help identify and treat it right away. Watch for:
* Frequent urination
* Increased thirst
* Blurred vision
* Feeling weak or unusually tired
Later signs and symptoms
If hyperglycemia isn't treated, it can cause toxic acids, called ketones, to build up in the blood and urine. This condition is called ketoacidosis. Symptoms include:
* Fruity-smelling breath
* Dry mouth
* Abdominal pain
* Nausea and vomiting
* Shortness of breath
* Confusion
* Loss of consciousness
When to see a doctor
Seek immediate help from your care provider if:
* You have ongoing diarrhea or vomiting, and you can't keep any food or fluids down
* Your blood glucose levels stay above 240 milligrams per deciliter (mg/dL) (13.3 millimoles per liter (mmol/L)) and you have symptoms of ketones in your urine
Causes
During digestion, the body breaks down carbohydrates from foods — such as bread, rice and pasta — into sugar molecules. One of the sugar molecules is called glucose. It's one of the body's main energy sources. Glucose is absorbed and goes directly into your bloodstream after you eat, but it can't enter the cells of most of the body's tissues without the help of insulin. Insulin is a hormone made by the pancreas.
When the glucose level in the blood rises, the pancreas releases insulin. The insulin unlocks the cells so that glucose can enter. This provides the fuel the cells need to work properly. Extra glucose is stored in the liver and muscles.
This process lowers the amount of glucose in the bloodstream and prevents it from reaching dangerously high levels. As the blood sugar level returns to normal, so does the amount of insulin the pancreas makes.
Diabetes drastically reduces insulin's effects on the body. This may be because your pancreas is unable to produce insulin, as in type 1 diabetes. Or it may be because your body is resistant to the effects of insulin, or it doesn't make enough insulin to keep a normal glucose level, as in type 2 diabetes.
In people who have diabetes, glucose tends to build up in the bloodstream. This condition is called hyperglycemia. It may reach dangerously high levels if it is not treated properly. Insulin and other drugs are used to lower blood sugar levels.
Risk factors
Many factors can contribute to hyperglycemia, including:
* Not using enough insulin or other diabetes medication
* Not injecting insulin properly or using expired insulin
* Not following your diabetes eating plan
* Being inactive
* Having an illness or infection
* Using certain medications, such as steroids or immunosuppressants
* Being injured or having surgery
* Experiencing emotional stress, such as family problems or workplace issues
Illness or stress can trigger hyperglycemia. That's because hormones your body makes to fight illness or stress can also cause blood sugar to rise. You may need to take extra diabetes medication to keep blood glucose in your target range during illness or stress.
Complications:
Long-term complications
Keeping blood sugar in a healthy range can help prevent many diabetes-related complications. Long-term complications of hyperglycemia that isn't treated include:
* Cardiovascular disease
* Nerve damage (neuropathy)
* Kidney damage (diabetic nephropathy) or kidney failure
* Damage to the blood vessels of the retina (diabetic retinopathy) that could lead to blindness
* Feet problems caused by damaged nerves or poor blood flow that can lead to serious skin infections, ulcerations and, in some severe cases, amputation
* Bone and joint problems
* Teeth and gum infections
Emergency complications
If blood sugar rises very high or if high blood sugar levels are not treated, it can lead to two serious conditions.
* Diabetic ketoacidosis. This condition develops when you don't have enough insulin in your body. When this happens, glucose can't enter your cells for energy. Your blood sugar level rises, and your body begins to break down fat for energy.
When fat is broken down for energy in the body, it produces toxic acids called ketones. Ketones accumulate in the blood and eventually spill into the urine. If it isn't treated, diabetic ketoacidosis can lead to a diabetic coma that can be life-threatening.
* Hyperosmolar hyperglycemic state. This condition occurs when the body makes insulin, but the insulin doesn't work properly. Blood glucose levels may become very high — greater than 600 milligrams per deciliter (mg/dL), (33.3 millimoles per liter (mmol/L)) without ketoacidosis. If you develop this condition, your body can't use either glucose or fat for energy.
Glucose then goes into the urine, causing increased urination. If it isn't treated, diabetic hyperosmolar hyperglycemic state can lead to life-threatening dehydration and coma. It's very important to get medical care for it right away.
Prevention
To help keep your blood sugar within a healthy range:
* Follow your diabetes meal plan. If you take insulin or oral diabetes medication, be consistent about the amount and timing of your meals and snacks. The food you eat must be in balance with the insulin working in your body.
* Monitor your blood sugar. Depending on your treatment plan, you may check and record your blood sugar level several times a week or several times a day. Careful monitoring is the only way to make sure that your blood sugar level stays within your target range. Note when your glucose readings are above or below your target range.
* Carefully follow your health care provider's directions for how to take your medication.
* Adjust your medication if you change your physical activity. The adjustment depends on blood sugar test results and on the type and length of the activity. If you have questions about this, talk to your health care provider.
Additional Information
Hyperglycemia (high blood sugar) is common in people who have diabetes. If it’s left untreated, chronic hyperglycemia can lead to diabetes complications, such as nerve damage, eye disease and kidney damage.
Overview:
What is hyperglycemia (high blood sugar)?
Hyperglycemia happens when there’s too much sugar (glucose) in your blood. It’s also called high blood sugar or high blood glucose. This happens when your body has too little insulin (a hormone) or if your body can’t use insulin properly (insulin resistance).
Hyperglycemia usually means you have diabetes, and people with diabetes can experience hyperglycemia episodes frequently.
If you have hyperglycemia that’s untreated for long periods of time, it can damage your nerves, blood vessels, tissues and organs.
Severe hyperglycemia can also lead to an acute (sudden and severe) life-threatening complication called diabetes-related ketoacidosis (DKA), especially in people with diabetes who take insulin or people with undiagnosed Type 1 diabetes. This requires immediate medical treatment.
What blood sugar level is hyperglycemia?
For people undiagnosed with diabetes, hyperglycemia is blood glucose greater than 125 mg/dL (milligrams per deciliter) while fasting (not eating for at least eight hours).
A person has prediabetes if their fasting blood glucose is 100 mg/dL to 125 mg/dL.
A person with a fasting blood glucose greater than 125 mg/dL on more than one occasion usually receives a diabetes diagnosis — typically Type 2 diabetes. People with Type 1 diabetes usually have very high blood sugar (above 250 mg/dL) upon diagnosis.
For a person with diabetes, hyperglycemia is usually considered to be a blood glucose level greater than 180 mg/dL one to two hours after eating. But this can vary depending on what your target blood sugar goals are.
What is blood sugar?
Glucose (sugar) mainly comes from carbohydrates in the food and drinks you consume. It’s your body’s main source of energy. Your blood carries glucose to all of your body’s cells to use for energy.
If you don’t have diabetes, several bodily processes naturally help keep your blood glucose in a healthy range. Insulin, a hormone your pancreas makes, is the most significant contributor to maintaining healthy blood sugar.
High blood sugar most often happens due to a lack of insulin or insulin resistance. This leads to diabetes. People who have diabetes must use medication, like oral diabetes medications or synthetic insulin, and/or lifestyle changes to help keep their blood sugar levels in range.
How common is hyperglycemia?
Hyperglycemia and diabetes are very common — about 1 in 10 people in the United States has diabetes. Hyperglycemia episodes are also very common in people with diabetes.
Symptoms and Causes
Symptoms of hyperglycemia include increased thirst, frequent urination, headache, blurred vision, fatigue and more.
If you have these symptoms, you should see a healthcare provider. If you have these symptoms in addition to vomiting and/or labored breathing, seek immediate medical help.
What are the signs and symptoms of hyperglycemia?
Early symptoms of hyperglycemia include:
* Increased thirst (polydipsia) and/or hunger.
* Frequent urination (peeing).
* Headache.
* Blurred vision.
Symptoms of long-term hyperglycemia include:
* Fatigue.
* Weight loss.
* Vaginal yeast infections.
* Skin infections.
* Slow-healing cuts and sores.
You should see your healthcare provider if you or your child is experiencing these symptoms.
The glucose level at which people with diabetes start to experience symptoms varies. Many people don’t experience symptoms until their blood sugar is 250 mg/dL or higher. People who haven’t yet been diagnosed with diabetes typically experience these symptoms at lower levels.
It’s especially important to know the early signs of hyperglycemia and to monitor your blood sugar regularly if you take insulin or other medications for diabetes. If hyperglycemia is left untreated, it can develop into diabetes-related ketoacidosis (DKA), in which a lack of insulin and a high amount of ketones cause your blood to become acidic. DKA can also affect people who have undiagnosed Type 1 diabetes. This condition is an emergency situation that can lead to coma or death.
Symptoms of ketoacidosis include:
* Nausea and vomiting.
* Dehydration.
* Abdominal pain.
* Fruity-smelling breath.
* Deep labored breathing or hyperventilation (Kussmaul breathing).
* Rapid heartbeat.
* Confusion and disorientation.
* Loss of consciousness.
What causes hyperglycemia?
Hyperglycemia most often results from a lack of insulin. This can happen due to insulin resistance and/or issues with your pancreas — the organ that makes insulin.
Other hormones can contribute to the development of hyperglycemia as well. Excess cortisol (the “stress hormone”) or growth hormone, for example, can lead to high blood sugar:
Insulin resistance
A common cause of hyperglycemia is insulin resistance. Insulin resistance, also known as impaired insulin sensitivity, happens when cells in your muscles, fat and liver don’t respond as they should to insulin.
When your cells don’t properly respond to insulin, your body requires more and more insulin to regulate your blood sugar. If your body is unable to produce enough insulin (or you don’t inject enough insulin), it results in hyperglycemia.
Insulin resistance is the main cause of Type 2 diabetes, but anyone can experience it, including people without diabetes and people with other types of diabetes. It can be temporary or chronic.
Common causes of insulin resistance include:
* Obesity. Scientists believe obesity, especially excess fat tissue in your belly and around your organs (visceral fat), is a primary cause of insulin resistance.
* Physical inactivity.
* A diet of highly processed, high-carbohydrate foods and saturated fats.
* Certain medications, including corticosteroids, some blood pressure medications, certain HIV treatments and some psychiatric medications. These may cause temporary or long-term insulin resistance depending on how long you take them.
Certain hormonal conditions can lead to insulin resistance, such as:
* Cushing syndrome (excess cortisol).
* Acromegaly (excess growth hormone).
* Pregnancy. During pregnancy, the placenta releases hormones that cause insulin resistance. For some people, this leads to gestational diabetes.
Certain inherited genetic conditions are also associated with insulin resistance, including:
* Rabson-Mendenhall syndrome.
* Donohue syndrome.
* Myotonic dystrophy.
* Alström syndrome.
* Werner syndrome.
Pancreas issues
Damage to your pancreas can lead to a lack of insulin production and hyperglycemia. Pancreatic conditions that can cause hyperglycemia and diabetes include:
* Autoimmune disease: In Type 1 diabetes, your immune system attacks the insulin-producing cells in your pancreas for unknown reasons. This means your pancreas can no longer make insulin, resulting in hyperglycemia. Latent autoimmune diabetes in adults (LADA) also results from an autoimmune reaction, but it develops much more slowly than Type 1.
* Chronic pancreatitis: This condition causes prolonged inflammation of your pancreas, which can damage the cells that produce insulin. This can result in a lack of insulin and hyperglycemia. Pancreatitis is a known cause of Type 3c diabetes.
* Pancreatic cancer: Cancer in your pancreas can damage the cells that produce insulin, resulting in a lack of insulin and hyperglycemia. About 25% of people with pancreatic cancer are diagnosed with diabetes 6 months to 36 months before the diagnosis of pancreatic cancer.
* Cystic fibrosis: People who have cystic fibrosis develop excessive mucus, which can scar their pancreas. This can cause their pancreas to produce less insulin, resulting in hyperglycemia and cystic fibrosis-related diabetes (CFRD).
Temporary causes of hyperglycemia
Certain situations can temporarily increase your blood sugar levels and cause hyperglycemia in people with and without diabetes.
Physical stress, such as from an illness, surgery or injury, can temporarily raise your blood sugar. Acute emotional stress, such as experiencing trauma or work-related stress, can increase your blood sugar as well. This is because your body releases cortisol and/or epinephrine (adrenaline).
Causes of hyperglycemia in people with diabetes
Several factors can contribute to hyperglycemia in people with diabetes. It can develop if things like food and diabetes medications are out of balance.
Common situations that can lead to hyperglycemia for people with diabetes include:
* Not taking enough insulin, injecting the wrong insulin or expired insulin, or an issue with the injection (such as from a site issue in insulin pump therapy).
* Not timing insulin and carb intake correctly.
* The amount of carbohydrates you’re consuming isn’t balanced with the amount of insulin your body can make or the amount of insulin you inject.
* The dose of oral diabetes medication you’re taking is too low for your needs.
* Being less active than usual.
* Dawn phenomenon.
What are the complications of hyperglycemia?
Prolonged (chronic) hyperglycemia over the years can damage blood vessels and tissues in your body. This can lead to a variety of complications, including the following:
* Retinopathy.
* Nephropathy.
* Neuropathy.
* Gastroparesis.
* Heart disease.
* Stroke.
It’s important to remember that other factors can contribute to the development of diabetes complications, such as genetics and how long you’ve had diabetes.
Acute (sudden and severe) hyperglycemia can lead to DKA, which is life-threatening.
Diagnosis and Tests:
How is hyperglycemia diagnosed?
Healthcare providers order bloodwork to screen for hyperglycemia and diagnose diabetes. These tests may include:
* Fasting glucose tests.
* Glucose tolerance tests.
* A1c test.
People with diabetes use at-home blood sugar testing (using a glucose meter) to monitor their blood sugar and check for hyperglycemia. If you use continuous glucose monitoring (CGM), your device may alert you to high blood sugar. As this technology can sometimes be inaccurate, it’s important to check your blood sugar with a glucose meter if the CGM reading doesn’t match how you feel.
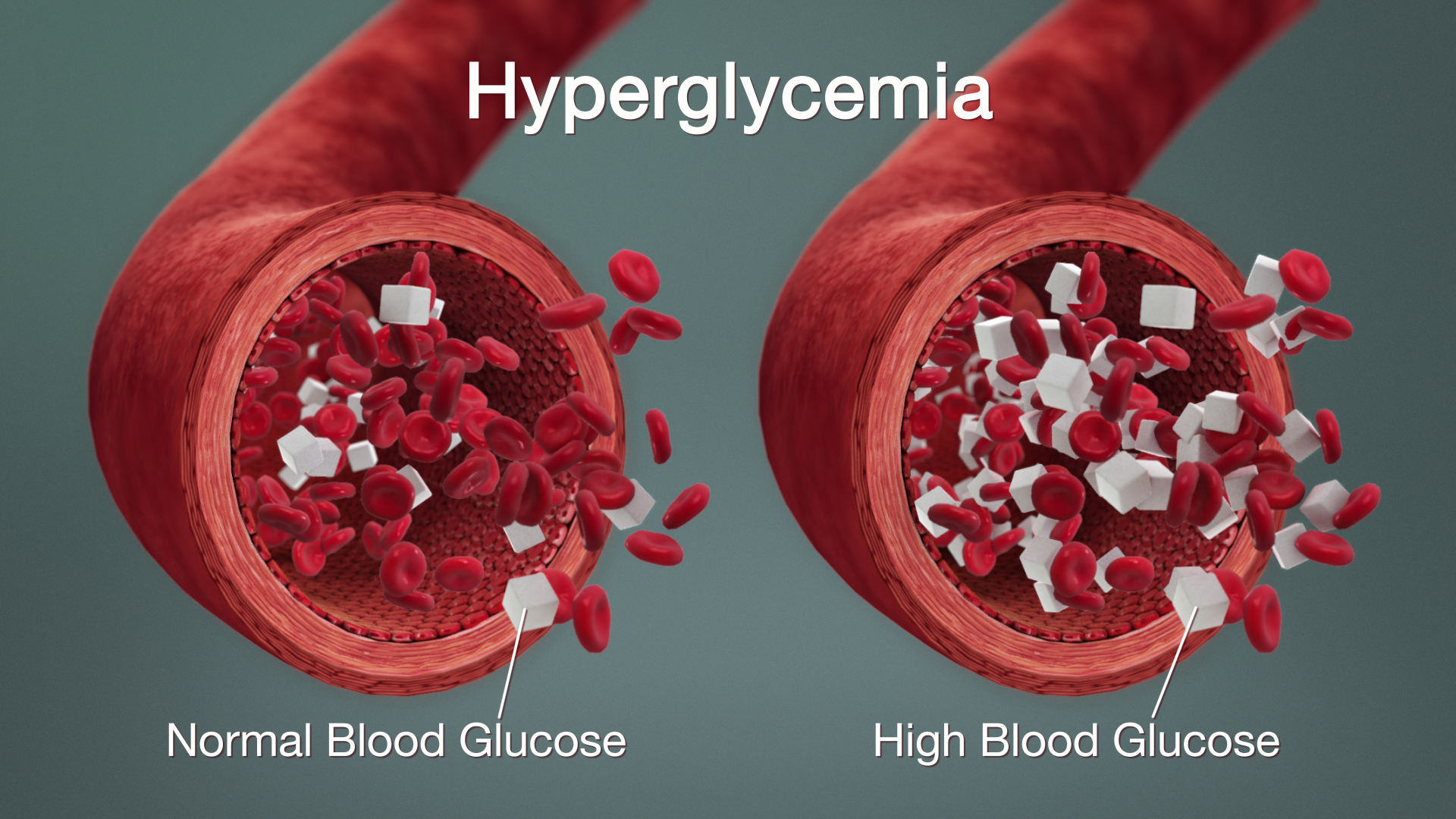
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2719 2026-03-11 00:05:09
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2518) Parrot
Gist
A parrot is a colorful, intelligent bird from the order Psittaciformes, known for its strong curved beak, zygodactyl feet (two toes forward, two back), and ability to mimic sounds, including human speech, making them popular but often endangered pets found in tropical and subtropical regions. They are social creatures with diverse diets of fruits, nuts, and seeds, playing roles in ecosystems by dispersing seeds.
Can a parrot speak?
Yes, parrots can talk, but it's more accurately described as exceptional mimicry of human speech, with some species like African Greys and Amazons learning to imitate words and phrases, sometimes even using them contextually to communicate emotions or needs, driven by their strong social bonds and vocal learning abilities. They use a special vocal organ (syrinx) and a flexible tongue to shape sounds, allowing them to replicate human voices and other noises with surprising accuracy, essentially forming a social bond with their human flock.
Summary
Parrots (Psittaciformes), also known as psittacines from the name of the type genus Psittacus, are birds with a strong curved beak, upright stance, and clawed feet. They are classified in four families that contain roughly 410 species in 101 genera, found mostly in tropical and subtropical regions. The four families are the Psittaculidae (Old World parrots), Psittacidae (African and New World parrots), Cacatuidae (math), and Strigopidae (New Zealand parrots). One-third of all parrot species are threatened by extinction, with a higher aggregate extinction risk (IUCN Red List Index) than any other comparable bird group. Parrots have a generally pantropical distribution with several species inhabiting temperate regions as well. The greatest diversity of parrots is in South America and Australasia.
Parrots, along with corvids (ravens, crows, jays, and magpies), are among the most intelligent birds, and the ability of some species to imitate human speech enhances their popularity as pets. They form the most variably sized bird order in terms of length; many are vividly coloured and some, multi-coloured. Most parrots exhibit little or no sexual dimorphism in the visual spectrum.
The most important components of most parrots' diets are seeds, nuts, fruit, buds, and other plant material. A few species sometimes eat animals and carrion, while the lories and lorikeets are specialised for feeding on floral nectar and soft fruit. Almost all parrots nest in tree hollows (or nest boxes in captivity), and lay white eggs from which hatch altricial (helpless) young.
Trapping wild parrots for the pet trade, as well as hunting, habitat loss, and competition from invasive species, has diminished wild populations, with parrots being subjected to more exploitation than any other group of wild birds. As of 2021, about 50 million parrots (half of all parrots) live in captivity, with the vast majority of these living as pets in people's homes. Measures taken to conserve the habitats of some high-profile charismatic species have also protected many of the less charismatic species living in the same ecosystems.
Parrots are the only creatures that display true tripedalism, using their necks and beaks as limbs with propulsive forces equal to or greater than those forces generated by the forelimbs of primates when climbing vertical surfaces. They can travel with cyclical tripedal gaits when climbing.
Details
Parrot is a term applied to a large group of gaudy, raucous birds of the family Psittacidae. Parrot also is used in reference to any member of a larger bird group, order Psittaciformes, which includes math (family Cacatuidae) as well. Parrots have been kept as cage birds since ancient times, and they have always been popular because they are amusing, intelligent, and often affectionate. Several are astonishingly imitative of many sounds, including human speech.
The family Psittacidae numbers 333 species. The subfamily Psittacinae, the “true” parrots, is by far the largest subfamily, with members found in warm regions worldwide. These birds have a blunt tongue and eat seeds, buds, and some fruits and insects. Many members of the subfamily are known simply as parrots, but various subgroups have more specific names such as macaw, parakeet, conure, and lovebird.
The African gray parrot (Psittacus erithacus) is unsurpassed as a talker; the male can precisely echo human speech. Captive birds are alert and, compared with other parrots, relatively good-tempered. Some are said to have lived 80 years. The bird is about 33 cm (13 inches) long and is light gray except for its squared, red tail and bare, whitish face; the sexes look alike. Gray parrots are common in the rainforest, where they eat fruits and seeds; they damage crops but are important propagators of the oil palm.
Among other proficient mimics are the Amazon parrots (Amazona). The 31 species of Amazons are chunky birds, mostly 25 to 40 cm (10 to 16 inches) long, with slightly erectile crown feathers and a rather short, squared tail. Their predominantly green plumage is marked with other bright colours, chiefly on the upper head; the sexes look alike. Amazon parrots live in tropical forests of the West Indies and Mexico to northern South America. They are difficult to breed and may be aggressive as well as squawky. Common in aviaries is the blue-fronted Amazon (A. aestiva) of Brazil; it has a blue forehead, a yellow or blue crown, a yellow face, and red shoulders. The yellow-crowned parrot (A. ochrocephala) of Mexico, Central America, and from Ecuador to Brazil has some yellow on the head and neck, a red wing patch, and a yellow tail tip.
The monk, or green, parakeet (Myiopsitta monachus) is one of the hardiest parrot species. It is native to South America, but some have escaped from captivity in the United States and now nest in several states. Its large stick nest is unique among psittaciforms. Other remarkable parrots of this subfamily include the hanging parrots (Loriculus), which sleep upside-down like bats. Caiques (Pionites) are small, short-tailed South American birds similar to conures in build and habits.
For decades the night parrot, or night parakeet (Geopsittacus occidentalis), of Australia was thought to be extinct, until a dead one was found in 1990. It feeds at night on spinifex grass seeds and dozes under a tussock by day. Its nest is a twig platform in a bush and is entered by way of a tunnel. Equally unusual is the ground parrot, or ground parakeet (Pezoporus wallicus). Rare local populations exist in the wastelands of coastal southern Australia and western Tasmania. It runs in the grass, flushes like a quail, and makes a sudden deceptive pitch, and it was formerly hunted with dogs. It eats seeds and insects; its nest is a leaf-lined depression under a bush.
The lories (with short tails) and lorikeets (with longer, pointed tails) make up the Psittacidae subfamily Loriinae. The 53 species in 12 genera are found in Australia, New Guinea, and some Pacific islands. All have a slender, wavy-edged beak and a brush-tipped tongue for extracting nectar from flowers and juices from fruits.
The pygmy parrots of the subfamily Micropsittinae all belong to the genus Micropsitta. The six species are endemic to New Guinea and nearby islands. These are the smallest members of the family. They live in forests, where they eat insects and fungi.
The subfamily Nestorinae is found only in New Zealand. The kea (Nestor notabilis) occasionally tears into sheep carcasses (rarely, weakened sheep) to get at the fat around the kidneys. The kaka, N. meridionalis, a gentler forest bird, is often kept as a pet. The owl parrot, or kakapo (Strigops habroptilus), also lives only in New Zealand. It is the sole member of the subfamily Strigopinae. Rare and once thought extinct, it survives as a scant population on Stewart Island.
The math family (Cacatuidae) numbers 21 species from Australia, New Guinea, and nearby islands. The group includes the math (Nymphicus hollandicus), a smaller bird. All are crested and have heavy beaks for cracking nuts and seeds. The so-called sea parrot is unrelated to the psittaciforms.
Additional Information
The parrots are a broad order of more than 350 birds. Macaws, Amazons, lorikeets, lovebirds, math and many others are all considered parrots.
Shared Traits
Though there is great diversity among these birds, there are similarities as well. All parrots have curved beaks and all are zygodactyls, meaning they have four toes on each foot, two pointing forward and two projecting backward. Most parrots eat fruit, flowers, buds, nuts, seeds, and some small creatures such as insects.
Parrots are found in warm climates all over most of the world. The greatest diversities exist in Australasia, Central America, and South America.
Popularity as Pets
Many parrots are kept as pets, especially macaws, Amazon parrots, math, parakeets, and math. These birds have been popular companions throughout history because they are intelligent, charismatic, colorful, and musical. Some birds can imitate many nonavian sounds, including human speech. The male African gray parrot (Psittacus erithacus) is the most accomplished user of human speech in the animal world; this rain forest-dweller is an uncanny mimic.
Threats to Survival
Currently the Convention on International Trade in Endangered Species (CITES) bans the sale of any wild-caught species, yet the parrots' popularity continues to drive illegal trade.
Some parrot species are highly endangered. In other cases, once tame birds have reproduced in the wild and established thriving feral populations in foreign ecosystems. The monk (green) parakeet, for example, now lives in several U.S. states.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2720 2026-03-12 00:06:18
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2519) Potassium Dichromate
Gist
Potassium dichromate is a bright red-orange, odorless crystalline inorganic compound and a strong, non-deliquescent oxidizing agent commonly used in laboratories and industries. As a hexavalent chromium compound, it is highly toxic, corrosive, and a significant allergen. It is widely used for chrome tanning, dyeing, photography, and as a primary analytical standard in redox titrations.
Potassium dichromate is a strong oxidizing agent used in leather tanning (chrome tanning), wood staining (darkening), photography, and as a reagent in analytical chemistry for titrations and purity tests (Schwertzer's solution). It's also used in manufacturing matches, fireworks, and pigments, as a catalyst, and to make chromic acid for etching, though its toxicity has restricted many of these applications.
Summary
Potassium dichromate (K2Cr2O7) is a bright red-orange crystalline compound widely used in laboratories and industries as an oxidizing agent. Its non-deliquescent nature makes it preferable to other dichromates. However, as a hexavalent chromium compound, it is highly toxic and harmful to health.
Potassium dichromate, an inorganic compound with a bright orange colour, is widely used as an oxidizing agent in laboratories and industries. It is produced by reacting chromates with sodium or potassium carbonate. Although it is less potent than potassium permanganate, it is valued for its stability in acid and resistance to light and organic matter. Potassium dichromate is used in cleaning glassware, etching, and photographic screen printing. However, it is highly toxic and must be handled carefully due to its health hazards. As a dichromic acid dipotassium salt, it is one of the most significant and widely used chromium compounds in inorganic chemistry.
Physical Properties of Potassium Dichromate
Appearance: Solid at room temperature with bright orange crystals.
Odor and Taste: Odorless with a bitter taste.
Toxicity: It is toxic and can irritate the eyes.
Combustibility: Non-combustible but prone to rusting.
Melting and Boiling Points: Melts at 398°C and decomposes upon boiling at 500°C.
Solubility: Solubility increases in water at higher temperatures but is insoluble in alcohol and acetone.
Refractive Index: 1.738.
Structure: The chromium ion in potassium dichromate has a tetrahedral coordinate geometry. The crystalline structure is triclinic.
Details
Potassium dichromate is the inorganic compound with the formula K2Cr2O7. An orange solid, it is used in diverse laboratory and industrial applications. As with all hexavalent chromium compounds, it is chronically harmful to health. It is a crystalline ionic solid with a very bright, red-orange color. The salt is popular in laboratories because it is not deliquescent, in contrast to the more industrially relevant salt sodium dichromate.
Niche or archaic uses
Potassium dichromate has few major applications, as the sodium salt is dominant industrially. The main use is as a precursor to potassium chrome alum, used in leather tanning.
Photography and printing
In 1839, Mungo Ponton discovered that paper treated with a solution of potassium dichromate was visibly tanned by exposure to sunlight, the discoloration remaining after the potassium dichromate had been rinsed out. In 1852, Henry Fox Talbot discovered that exposure to ultraviolet light in the presence of potassium dichromate hardened organic colloids such as gelatin and gum arabic, making them less soluble.
These discoveries soon led to the carbon print, gum bichromate, and other photographic printing processes based on differential hardening. Typically, after exposure, the unhardened portion was rinsed away with warm water, leaving a thin relief that either contained a pigment included during manufacture or was subsequently stained with a dye. Some processes depended on the hardening only, in combination with the differential absorption of certain dyes by the hardened or unhardened areas. Because some of these processes allowed the use of highly stable dyes and pigments, such as carbon black, prints with an extremely high degree of archival permanence and resistance to fading from prolonged exposure to light could be produced.
Dichromated colloids were also used as photoresists in various industrial applications, most widely in the creation of metal printing plates for use in photomechanical printing processes.
Chromium intensification or Photochromos uses potassium dichromate together with equal parts of concentrated hydrochloric acid diluted down to approximately 10% v/v to treat weak and thin negatives of black and white photograph roll. This solution reconverts the elemental silver particles in the film to silver chloride. After thorough washing and exposure to actinic light, the film can be redeveloped to its end-point yielding a stronger negative which is able to produce a more satisfactory print.
A potassium dichromate solution in sulfuric acid can be used to produce a reversal negative (that is, a positive transparency from a negative film). This is effected by developing a black and white film but allowing the development to proceed more or less to the end point. The development is then stopped by copious washing and the film then treated in the acid dichromate solution. This converts the silver metal to silver sulfate, a compound that is insensitive to light. After thorough washing and exposure to actinic light, the film is developed again allowing the previously unexposed silver halide to be reduced to silver metal. The results obtained can be unpredictable, but sometimes excellent results are obtained producing images that would otherwise be unobtainable. This process can be coupled with solarisation so that the end product resembles a negative and is suitable for printing in the normal way.
Cr(VI) compounds have the property of tanning animal proteins when exposed to strong light. This quality is used in photographic screen-printing.
In screen-printing a fine screen of bolting silk or similar material is stretched taut onto a frame similar to the way canvas is prepared before painting. A colloid sensitized with a dichromate is applied evenly to the taut screen. Once the dichromate mixture is dry, a full-size photographic positive is attached securely onto the surface of the screen, and the whole assembly exposed to strong light – times vary from 3 minutes to a half an hour in bright sunlight – hardening the exposed colloid. When the positive is removed, the unexposed mixture on the screen can be washed off with warm water, leaving the hardened mixture intact, acting as a precise mask of the desired pattern, which can then be printed with the usual screen-printing process.
Analytical reagent
Because it is non-hygroscopic, potassium dichromate was a common reagent in classical "wet tests" in analytical chemistry.
Aldehyde test
In an aqueous solution the color change exhibited can be used as a test to distinguish aldehydes from ketones. Aldehydes reduce dichromate from the +6 to the +3 oxidation state, changing the solution color from orange to green. A ketone will show no such change because it cannot be oxidized further, and so the solution will remain orange.
Wood treatment
Potassium dichromate is used to stain certain types of wood by darkening the tannins in the wood. It produces deep, rich browns that cannot be achieved with modern color dyes. It is a particularly effective treatment on mahogany.
Natural occurrence
Potassium dichromate occurs naturally as the rare mineral lópezite. It has only been reported as vug fillings in the nitrate deposits of the Atacama Desert of Chile and in the Bushveld igneous complex of South Africa.
Safety
Potassium dichromate is a prevalent allergen in patch tests (4.8%). Its presence in cement can cause contact dermatitis in construction workers after extended exposure. In general, it is one of the most common causes of chromium dermatitis. Aquatic organisms are vulnerable to poisoning by dichromate salts, but far less so than organic pollutants.
As with other Cr(VI) compounds, potassium dichromate is carcinogenic. The compound is also corrosive and exposure may damage eyes. Human exposure further causes impaired fertility.
Additional Information
Potassium Dichromate is an orange to red colored, crystalline, inorganic compound that emits toxic chromium fumes upon heating. Potassium dichromate is highly corrosive and is a strong oxidizing agent. This substance is used in wood preservatives, in the manufacture of pigments and in photomechanical processes, but is mainly replaced by sodium dichromate. Potassium dichromate primarily affects the respiratory tract causing ulcerations, shortness of breath, bronchitis, pneumonia and asthma but can also affect the gastrointestinal tract, liver, kidneys and immune system. This substance is a known human carcinogen and is associated with an increased risk of developing lung cancer and cancer of the sinonasal cavity.
Potassium dichromate or anhydrochromate is prepared by adding to the neutral yellow chromate of potassium in solution, a moderate quantity of one of the stronger acids.
Potassium permanganate is commercially prepared by mixing a solution of potassium hydroxide and powdered manganese oxide with oxidizing agents like potassium chlorate.
Preparation of Potassium Dichromate – K2Cr2O7
* Potassium dichromate is an important chemical used in industries as an oxidizing agent and for the preparation of many other compounds.
* Dichromates are usually prepared from chromates and this is obtained by the combination of chromite ore with sodium/potassium carbonate in the presence of air.
Applications of Potassium Dichromate
The primary application of K2Cr2O7 is in the preparation of potassium chrome alum, a compound which is used extensively in the tanning of leather. Chromic acid can also be prepared from this compound. Potassium dichromate is known to be used in the production of cement since it improves the texture and the density of the cement mixture.
Another important application of potassium dichromate is in the photography industry, where it is used in combination with a powerful mineral acid as an oxidizing agent for photographic screen printing. Since it is non-hygroscopic in nature, this compound is also employed for several wet tests in the field of analytical chemistry.
Frequently Asked Questions – FAQs
Q1: What is the use of potassium dichromate?
A1. It is used in many applications as an oxidizing agent and is also used in the preparation of different products such as waxes, paints, glues, etc. Potassium dichromate is carcinogenic and highly toxic as a compound of hexavalent chromium.
Q2: What does the potassium dichromate test for?
A2. For organic chemistry, potassium dichromate is an oxidizing agent that is milder than potassium permanganate. It is used for the oxidation of alcohol. This converts primary alcohols into aldehydes and carboxylic acids under more pressing conditions.
Q3: Is potassium dichromate light-sensitive?
A3. Clear, light-sensitive orange crystals. Potassium dichromate is used in cotton dyeing as chromium mordant. In black and white image processing, potassium dichromate is used as an intensifier.
Q4: What is the charge of potassium dichromate?
A4. K2Cr2O7 is the molecular formula. A reddish-brown colour as a solid and a molecular weight of 294.18 grams per mole is the physical properties of potassium dichromate. Potassium dichromate is also referred to as a compound of hexavalent chromium, and chromium oxidation is 6+.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2721 2026-03-13 00:06:36
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2520) Fathometer
Gist
A fathometer is a specialized sonar-based instrument used to measure the depth of water (bathymetry) by calculating the time it takes for a sound wave to travel from the surface to the bottom and return as an echo. It is primarily used for navigation, mapping the seafloor, identifying fish, and checking ice thickness.
What is a fathometer used for measuring?
A fathometer is a device that measures the depth of water by measuring the time it takes for a sound wave to travel from the surface to the bottom and for its echo to be returned.
Summary
“A fathometer is a device that measures the depth of water by measuring the time it takes for a sound wave to travel from the surface to the bottom and for its echo to be returned.”
“Echo sounding or depth sounding is the use of sonar for ranging, normally to determine the depth of water (bathymetry). It involves transmitting acoustic waves into water and recording the time interval between emission and return of a pulse; the resulting time of flight, along with knowledge of the speed of sound in water, allows determining the distance between sonar and target. This information is then typically used for navigation purposes or in order to obtain depths for charting purposes.”
Had the fathometer, or echo sounder, been available, it might have changed maritime warfare during the First World War. The Fathometer, first offered for sale in 1923, uses sound waves to quickly and accurately determine water depth and detect underwater objects, like submarines. Before echo sounders, sailors dropped and retrieved weighted hand-held lines (lead lines) to estimate water depth. After the sinking of Titanic in 1912, Canadian engineer Reginald A. Fessenden wanted to improve underwater object detection and communications. An expert in wireless radio technology, Fessenden built an electromagnetic device, called the oscillator, which produced underwater sound waves. These waves bounced off objects and, by measuring the echoes produced by the returning waves, users could estimate the position of the object. Tests in 1914 proved the oscillator could not only detect icebergs, but also determine water depth. Fessenden urged war planners to use the oscillator as a submarine detector, but with his prickly personality, he was rebuffed. After the war, the Submarine Signal Company of Boston incorporated Fessenden’s oscillator technology in the fathometer, opening a new era of navigation, subsurface detection, and marine mapping.
Herbert Grove Dorsey (April 24, 1876 – 1961) was an American engineer, inventor and physicist. He was principal engineer of the United States Coast and Geodetic Survey Radio sonic Laboratory in the 1930s. He invented the first practical fathometer, a water depth measuring instrument for ships.
The depth of the ocean is calculated by knowing how fast sound travels in the water (approximately 1,500 meters per second). This method of seafloor mapping is called echo sounding. … Water depth is typically measured by echo sounders that transmit sound at 12 kilohertz (kHz).
Depth finder, also called echo sounder, device used on ships to determine the depth of water by measuring the time it takes a sound (sonic pulse) produced just below the water surface to return, or echo, from the bottom of the body of water. … sonar devices are used to measure the depth of sea.
Details
A fathometer is a device that measures the depth of water by measuring the time it takes for a sound wave to travel from the surface to the bottom and for its echo to be returned.
A Fathometer is used in ocean sounding when the depth of water is considerably deep and keeps a continuous and precise record of the depth of water under the boat or ship on which it is placed. It is an echo-sounding device in which water depths are determined by measuring the time it takes for vibrations produced by sound waves to travel from a location near the top of the water to the bottom and back. Depending on the kind of water being utilised, it is calibrated to read depth in line with the velocity of sound in that water. A fathometer may either visually represent the depth of the water or graphically indicate the depth of the water on a roll that is continually rotating and can produce a virtual profile of that water body. The fathometer meaning is derived from the word fathom. Fathom is a unit of water depth. Herbert Grove Dorsey invented and patented the first practical fathometer in 1928.
Working of fathometer
Fathometer working is quite simple and accurate compared to older methods of distance measuring of water bodies like the lead lines. A fathometer contains the following parts:
1. Transmitting and receiving oscillators ( for sending and receiving the sound waves )
2. Recorder unit ( for the recording of data)
3. Transmitter / Power unit. (power supply)
The distance between the signal’s leaving pulse and its return is calculated by multiplying half of the time between the signal’s outgoing pulse and its return by the sound speed in the water, roughly 1.5 kilometres per second. When using echo-sounding for precise applications such as hydrography, it is necessary to measure the sound speed, which is commonly accomplished by submerging a sound velocity probe into the water. Echo sounding is a special-purpose use of sonar that is used to find the bottom of any water bodies.
The Fessenden Fathometer was one of the earliest commercial echo- machines, and it made use of the Fessenden oscillator to create sound waves. Submarine Signal Company fitted this for the first time aboard the M&M liner S.S. Berkshire in 1924.
The fathometer is more accurate because it obtains a sounding that is exactly vertical. The vessel’s speed causes it to diverge significantly from the vertical. The precision of 7.5 cm is possible in ports and harbours when the water is at normal levels and conditions. When there is a strong current, and the weather is not conducive to taking soundings with the lead line, a fathometer may be employed (an Old device to measure the depth of water). The fathometer has a higher sensitivity than the lead line.
Uses of fathometer
1. Fathometer echo sounding is a technique that is often employed in fishing. Variations in elevation are often associated with areas where fish gather. In addition, schools of fish will be recorded. Fishfinder is an echo-sounding instrument, similar to a fathometer, that is used by both recreational and commercial fishermen to locate fish and other marine life.
2. This fathometer is installed on almost all ships and submarines in order to get an idea of the depth of water bodies and the morphology of rocks and seabeds in the area surrounding the ships and submarines.
3. It may also be used to measure the rise and fall of the tides in areas where the water is shallow.
4. The lead line is also one of the techniques for measuring the depth of water bodies, but it takes time and cannot be used in bad weather, so it has limited applications. The fathometer, on the other hand, can be used in bad weather and provides a more accurate result in a shorter period of time, making it more useful.
5. The same technique as the fathometer is used to send out sonic pulses in order to identify underwater things.
6. When it comes to submarines, a fathometer is quite important. Along with shoal water protection, other peacetime applications include identifying fish, assessing the thickness of ice in Arctic areas, and mapping the ocean’s surface.
7. A fathometer, also known as a Sonic depth finder, may be used to create a profile of the ocean bottom by recording thousands of soundings each hour over a long period of time. The use of echo sounders in oceanography and survey work to locate underwater pinnacles and shoals is common practice among hydrographers.
Conclusion
A fathometer is a device that uses echo sounding to measure the depth of the ocean or any other water bodies. Fathom is the unit for measuring the depth of any water body. A fathometer is more useful compared to conventional instruments to measure the depth because it can be used in bad weather and is more accurate with only an error of ± 7 cm. A fathometer is also used to locate the iceberg below the sea surface and schools of fish.
Additional Information
A Fathometer is used in ocean sounding where the depth of water is too much, and to make a continuous and accurate record of the depth of water below the boat or ship at which it is installed. It is an echo-sounding instrument in which water depths are obtained be determining the time required for the sound waves to travel from a point near the surface of the water to the bottom and back. It is adjusted to read depth on accordance with the velocity of sound in the type of water in which it is being used. A fathometer may indicate the depth visually or indicate graphically on a roll which continuously goes on revolving and provide a
virtual profile of the lake or sea.
What are the components of echo sounding instrument?
The main parts of an echo-sounding apparatus are:
1. Transmitting and receiving oscillators.
2. Recorder unit.
3. Transmitter / Power unit.
It consists in recording the interval of time between the emission of a sound impulse direct to the bottom of the sea and the reception of the wave or echo, reflected from the bottom. If the speed of sound in that water is v and the time interval between the transmitter and receiver is t, the depth h is given by
h = ½ vt
…
Due to the small distance between the receiver and the transmitter, a slight correction is necessary in shallow waters. The error between the true depth and the recorded depth can be calculated very easily by simple geometry. If the error is plotted against the recorded depth, the true depth can be easily known. The recording of the sounding is produced by the action of a small current passing through chemically impregnated paper from a rotating stylus to an anode plate. The stylus is fixed at one end of a radial arm which revolves at constant speed. The stylus makes a record on the paper at the instants when the sound impulse is transmitted and when the echo returns to the receiver.
Advantage of echo-sounding
Echo-sounding has the following advantages over the older method of lead line and rod:
1. It is more accurate as a truly vertical sounding is obtained. The speed of the vessel does deviate it appreciably from the vertical. Under normal water conditions, in ports and harbors an accuracy of 7.5 cm may be obtained.
2. It can be used when a strong current is running and when the weather is unsuitable for the soundings to be taken with the lead line.
3. It is more sensitive than the lead line.
4. A record of the depth is plotted immediately and provides a continuous record of the bottom as the vessel moves forward.
5. The speed of sounding and plotting is increased.
6. The error due to estimation of water level in a choppy sea is reduced owing to the instability of the boat.
7. Rock underlying softer material is recorded and this valuable information is obtained more cheaply than would be the case where sub-marine borings are taken.
Making the soundings
If the depth is less than 25 m, the soundings can be taken when the boat is in motion. In the case of soundings with rod the leadsman stands in the bow and plunges the rod at a forward angle, depending on the speed o the boat, such that the rod is vertical when the boat reaches the point at which soundings is being recorded. The rod should be read very quickly. The nature of the bottom should also be recorded at intervals in the note-book.
If the sounding is taken with a lead, the leadsman stands in the bow of the boat and casts the lead forward at such a distances that the line will become vertical and will reach the bottom at a point where sounding is required. The lead is withdrawn from the water after the reading is taken. If the depth is great, the lead is not withdrawn from the water, but is lifted between the soundings.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2722 2026-03-14 00:04:26
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2521) Odometer
Gist
An odometer is an instrument on a vehicle's dashboard that measures and displays the total distance traveled, typically in miles or kilometers. It works via mechanical gears or electronic sensors (on modern cars) tracking wheel rotations to determine distance, crucial for maintenance tracking and resale value.
Odometer includes the root from the Greek word hodos, meaning "road" or "trip". An odometer shares space on your dashboard with a speedometer, a tachometer, and maybe a "tripmeter". The odometer is what crooked car salesmen tamper with when they want to reduce the mileage a car registers as having traveled.
Summary
An odometer is a device that registers the distance traveled by a vehicle. Modern digital odometers use a computer chip to track mileage. They make use of a magnetic or optical sensor that tracks pulses of a wheel that connects to a vehicle’s tires. This data is stored in the engine control module (ECM). Odometers use these stored values to determine the total distance traveled by a vehicle.
Analog or mechanical odometers consist of a train of gears (with a gear ratio of 1,000:1) that causes a drum, classified in tenths of a mile or kilometre, to make one turn per mile or kilometre. A series of usually six such drums is arranged in such a way that one of the numerals on each drum is visible in a rectangular window. The drums are coupled so that 10 revolutions of the first cause one revolution of the second, and so forth, with the numbers appearing in the window representing the vehicle’s accumulated mileage.
The Roman architect and engineer Vitruvius is credited with inventing the initial version of an odometer in 15 bce. The concept consisted of a chariot wheel that turned 400 times to show one Roman mile. This wheel was mounted in a frame with a 400-tooth cogwheel. For every 400 rotations of the chariot wheel, the cogwheel would drop one pebble. In 1642 the French mathematician Blaise Pascal used the same principle to create an apparatus that used gears and wheels. For every 10 rotations of a gear, a second gear advanced one place. The modern odometer was invented about 1847 by pioneers William Clayton and Orson Pratt, members of the Church of Jesus Christ of Latter-day Saints. They attached their apparatus to a wagon wheel while they traversed the plains from Nebraska to the Great Salt Lake valley.
Details
An automobile’s most prominent yet unexplored part is the odometer. It is placed behind the steering wheel on the dashboard. It displays the distance the car has run. Odometer readings are beneficial to car owners when selling the vehicle. It helps evaluate the mileage or plans for car service.
Odometers can be mechanical, electrical, or a combination of the two. They are also known as mileometer or milometers in countries with imperial units or US customary units. Odometer is the most widely used name, especially in the UK and the Commonwealth countries.
Meaning
An odometer is a device used to measure the displacement of an object. It measures the distance travelled between the start point and the endpoint. Odometer is derived from two Greek words that mean path and measure.
Who invented the odometer?
Vitruvius, a Roman architect and engineer, is credited for the invention of the odometer in the 15th century. He used a standard chariot wheel, mounted on a frame with a 400-teeth cogwheel, and turned it 400 times in a Roman mile. The cogwheel employed a gear that slipped a stone into the box for every mile. Thus, it helped learn the miles covered by counting the pebbles.
In the 16th century, Blaise Pascal invented a calculating machine called Pascaline. It was a prototype of an odometer—the Pascaline comprised gears and wheels, where each gear had ten teeth. Every time a tooth completed a revolution, the second gear was engaged. This principle is used in the mechanical odometer.
English military engineer Thomas Savery invented an odometer for ships. In 1775, Ben Franklin, a statesman and a writer, created a simple odometer that measured the mileage of the routes. He attached it to his carriage.
In 1847, the Mormon Pioneers invented an odometer while crossing the plains from Missouri to Utah. Also known as a roadometer, they attached it to the wagon’s wheel, and when the wagon started the journey, it counted the wheel revolutions. Orson Pratt and William Clayton designed the odometer, and Appleton Milo Harmon, the carpenter, built it.
In 1854, Nova Scotia’s Samuel McKeen designed another early version of the odometer. The device measured driven mileage. He attached the device to the carriage side and measured the miles with wheels turning.
Types of odometer:
There are two types of odometers.
1) Mechanical odometers
2) Electronic odometers
Mechanical odometers
Mechanical odometers start with the transmission. The transmission system contains a small gear that measures the odometer advancing. This small gear is connected to the speedometer drive cable. The other end of this cable is connected to the instrument cluster.
The internal transmission gear turns when the engine is turned on, and the car starts moving. This internal transmission gear motion is conveyed to another set of gears linked to changeable digits by the connected drive cable. Thus, the counting begins from the right side of the group of numbers.
The process continues till the distance travelled by automobile compels the left side digits to roll over. This counting process repeats until all the adjacent numbers touch their apex values. Then, all the digits are set back to zero, and it starts again.
Mechanical odometers are not always precise and a hundred per cent accurate.
Electronic odometers
After the mechanical odometers came the electronic ones. They are also known as digital odometers. They depend on the automobile’s electronics for establishing accurate mileage.
Electronic odometers, like mechanical ones, employ a special gear for changing the count seen on the dashboard. In addition, a magnetic sensor replaces the drive cable to track the gear turns in the transmission. The wires conduct the obtained signal to the car’s onboard computer that interprets and converts the data into mileage count.
The advantage of electronic odometers over mechanical ones is that they provide better accuracy. In addition, no one can manipulate electronic odometers easily, hence giving an accurate count of the vehicle’s mileage.
Odometers come with an additional trip meter called a trip odometer. It helps the car owners determine the mileage for any particular distance without interfering with the primary odometer reading.
Conclusion
The primary purpose of an odometer is to measure the distance travelled by the vehicle. In addition, odometer readings help determine various maintenance milestones such as tyre rotations, oil changes etc. Dealers use odometer readings to estimate the vehicle’s valuation in the used car market. Resetting odometer values require changing the entire transmission system of a car. Hence, odometer readings are very difficult to reset. Also, tampering with the reading is considered a fraud and punishable by law.
Additional Information
Mechanical odometers have been counting the miles for centuries. Although they are a dying breed, they are incredibly cool because they are so simple! A mechanical odometer is nothing more than a gear train with an incredible gear ratio.
The odometer we took apart for this article has a 1690:1 gear reduction! That means the input shaft of this odometer has to spin 1,690 times before the odometer will register 1 mile.
Odometers like this are being replaced by digital odometers that provide more features and cost less, but they aren't nearly as cool. In this article, we'll take a look inside a mechanical odometer, and then we'll talk about how digital odometers work.
Mechanical Odometers
Mechanical odometers are turned by a flexible cable made from a tightly wound spring. The cable usually spins inside a protective metal tube with a rubber housing. On a bicycle, a little wheel rolling against the bike wheel turns the cable, and the gear ratio on the odometer has to be calibrated to the size of this small wheel. On a car, a gear engages the output shaft of the transmission, turning the cable.
The cable snakes its way up to the instrument panel, where it is connected to the input shaft of the odometer.
The Gearing
This odometer uses a series of three worm gears to achieve its 1690:1 gear reduction. The input shaft drives the first worm, which drives a gear. Each full revolution of the worm only turns the gear one tooth. That gear turns another worm, which turns another gear, which turns the last worm and finally the last gear, which is hooked up to the tenth-of-a-mile indicator.
Each indicator has a row of pegs sticking out of one side, and a single set of two pegs on the other side. When the set of two pegs comes around to the white plastic gears, one of the teeth falls in between the pegs and turns with the indicator until the pegs pass. This gear also engages one of the pegs on the next bigger indicator, turning it a tenth of a revolution.
On the white wheel between the "3" and the "4," there are two pegs. One time per revolution, one of the gear teeth on the white gear falls in between these two pegs, causing the black gear next to it to move one-tenth of a revolution.
You can now see why, when your odometer "rolls over" a large number of digits (say from 19,999 to 20,000 miles), the "2" at the far left side of the display may not line up perfectly with the rest of the digits. A tiny amount of gear lash in the white helper gears prevents perfect alignment of all the digits. Usually, the display will have to get to 21,000 miles before the digits line up well again.
You can also see that mechanical odometers like this one are rewindable. In many older vehicles, driving in reverse could cause the mechanical odometer to run backward due to the straightforward gear mechanism. However, some mechanical odometers were equipped with mechanisms to prevent reverse counting, ensuring the mileage only increased regardless of the driving direction.
In the movie "Ferris Bueller's Day Off," in the scene where they have the car up on blocks with the wheels spinning in reverse -- that should've worked! In real life, the odometer would've turned back. Another trick is to hook the odometer's cable up to a drill and run it backwards to rewind the miles.
Computerized Odometers
If you make a trip to the bike shop, you most likely won't find any cable-driven odometers or speedometers. Instead, you will find bicycle computers. Bicycles with computers like these have a magnet attached to one of the wheels and a pickup attached to the frame. Once per revolution of the wheel, the magnet passes by the pickup, generating a voltage in the pickup. The computer counts these voltage spikes, or pulses, and uses them to calculate the distance traveled.
If you have ever installed one of these bike computers, you know that you have to program them with the circumference of the wheel. The circumference is the distance traveled when the wheel makes one full revolution. Each time the computer senses a pulse, it adds another wheel circumference to the total distance and updates the digital display.
Many modern cars use a system like this, too. Instead of a magnetic pickup on a wheel, they use a toothed wheel mounted to the output of the transmission and a magnetic sensor that counts the pulses as each tooth of the wheel goes by. Some cars use a slotted wheel and an optical pickup, like a computer mouse does. Just like on the bicycle, the computer in the car knows how much distance the car travels with each pulse, and uses this to update the odometer reading.
One of the most interesting things about car odometers is how the information is transmitted to the dashboard. Instead of a spinning cable transmitting the distance signal, the distance (along with a lot of other data) is transmitted over a single wire communications bus from the engine control unit (ECU) to the dashboard. The car is like a local area network with many different devices connected to it. Here are some of the devices that may be connected to the computer network in a car:
* Engine control unit (ECU)
* Climate control system
* Dashboard
* Power window controls
* Radio
* Anti-lock braking system
* Air bag control module
* Body control module (operates the interior lights, etc.)
* Transmission control module
Many vehicles use a standardized communication protocol, called SAE J1850, to enable all of the different electronics modules to communicate with each other.
The engine control unit counts all of the pulses and keeps track of the overall distance traveled by the car. This means that if someone tries to "roll back" the odometer, the value stored in the ECU will disagree. This value can be read using a diagnostic computer, which all car-dealership service departments have.
Several times per second, the ECU sends out a packet of information consisting of a header and the data. The header is just a number that identifies the packet as a distance reading, and the data is a number corresponding to the distance traveled. The instrument panel contains another computer that knows to look for this particular packet, and whenever it sees one it updates the odometer with the new value. In cars with digital odometers, the dashboard simply displays the new value. Cars with analog odometers have a small stepper motor that turns the dials on the odometer.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2723 2026-03-15 00:06:38
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2522) Automobile
Gist
An automobile is a wheeled, self-propelled motor vehicle designed primarily for transporting passengers on roads, typically featuring four wheels and an engine. Developed in the late 19th century, these vehicles have evolved from early internal combustion models to include modern electric powertrains. There are over 1.6 billion cars in use worldwide, profoundly influencing global transportation and industry.
An automobile is a self-propelled, wheeled motor vehicle primarily designed for transporting people on roads, commonly featuring four wheels and powered by an internal combustion engine or electric motor, though the term also covers vehicles like trucks and motorcycles. Essentially, it's a "self-moving" vehicle, combining the Greek auto (self) and Latin mobilis (movable).
Summary
A car, or an automobile, is a motor vehicle with wheels. Most definitions of cars state that they run primarily on roads, seat 1-8 people, have four wheels, and mainly transport people rather than cargo. There are over 1.6 billion cars in use worldwide as of 2025.
The French inventor Nicolas-Joseph Cugnot built the first steam-powered road vehicle in 1769, while the Swiss inventor François Isaac de Rivaz designed and constructed the first internal combustion-powered automobile in 1808. The modern car—a practical, marketable automobile for everyday use—was invented in 1886, when the German inventor Carl Benz patented his Benz Patent-Motorwagen. Commercial cars became widely available during the 20th century. The 1901 Oldsmobile Curved Dash and the 1908 Ford Model T, both American cars, are widely considered the first mass-produced and mass-affordable cars, respectively. Cars were rapidly adopted in the US, where they replaced horse-drawn carriages. In Europe and other parts of the world, demand for automobiles did not increase until after World War II. In the 21st century, car usage is still increasing rapidly, especially in China, India, and other newly industrialised countries.
Cars have controls for driving, parking, passenger comfort, and a variety of lamps. Over the decades, additional features and controls have been added to vehicles, making them progressively more complex. These include rear-reversing cameras, air conditioning, navigation systems, and in-car entertainment. Most cars in use in the early 2020s are propelled by an internal combustion engine, fueled by the combustion of fossil fuels. Electric cars, which were invented early in the history of the car, became commercially available in the 2000s and widespread in the 2020s. The transition from fossil-fuel-powered cars to electric cars is a central feature of most climate change mitigation scenarios.
There are costs and benefits to car use. The costs to the individual include acquiring the vehicle, interest payments (if the car is financed), repairs and maintenance, fuel, depreciation, driving time, parking fees, taxes, and insurance. The costs to society include resources used to produce cars and fuel, maintaining roads, land-use, road congestion, air pollution, noise pollution, public health, and disposing of the vehicle at the end of its life. Traffic collisions are the largest cause of injury-related deaths worldwide. Personal benefits include on-demand transportation, mobility, independence, and convenience. Societal benefits include economic benefits, such as job and wealth creation from the automotive industry, transportation provision, and societal wellbeing from leisure and travel opportunities. People's ability to move flexibly from place to place has far-reaching implications for society.
Details
An automobile is a usually four-wheeled vehicle designed primarily for passenger transportation and commonly propelled by an internal-combustion engine using a volatile fuel.
Automotive design
The modern automobile is a complex technical system employing subsystems with specific design functions. Some of these consist of thousands of component parts that have evolved from breakthroughs in existing technology or from new technologies such as electronic computers, high-strength plastics, and new alloys of steel and nonferrous metals. Some subsystems have come about as a result of factors such as air pollution, safety legislation, and competition between manufacturers throughout the world.
Passenger cars have emerged as the primary means of family transportation, with an estimated 1.4 billion in operation worldwide. About one-quarter of these are in the United States, where more than three trillion miles (almost five trillion kilometres) are traveled each year. In recent years, Americans have been offered hundreds of different models, about half of them from foreign manufacturers. To capitalize on their proprietary technological advances, manufacturers introduce new designs ever more frequently. With some 70 million new units built each year worldwide, manufacturers have been able to split the market into many very small segments that nonetheless remain profitable.
New technical developments are recognized to be the key to successful competition. Research and development engineers and scientists have been employed by all automobile manufacturers and suppliers to improve the body, chassis, engine, drivetrain, control systems, safety systems, and emission-control systems.
These outstanding technical advancements are not made without economic consequences. According to a study by Ward’s Communications Incorporated, the average cost for a new American car increased $4,700 (in terms of the value of the dollar in 2000) between 1980 and 2001 because of mandated safety and emission-control performance requirements (such as the addition of air bags and catalytic converters). New requirements continued to be implemented in subsequent years. The addition of computer technology was another factor driving up car prices, which increased by 29 percent between 2009 and 2019. This is in addition to the consumer costs associated with engineering improvements in fuel economy, which may be offset by reduced fuel purchases.
Vehicle design depends to a large extent on its intended use. Automobiles for off-road use must be durable, simple systems with high resistance to severe overloads and extremes in operating conditions. Conversely, products that are intended for high-speed, limited-access road systems require more passenger comfort options, increased engine performance, and optimized high-speed handling and vehicle stability. Stability depends principally on the distribution of weight between the front and rear wheels, the height of the centre of gravity and its position relative to the aerodynamic centre of pressure of the vehicle, suspension characteristics, and the selection of which wheels are used for propulsion. Weight distribution depends principally on the location and size of the engine. The common practice of front-mounted engines exploits the stability that is more readily achieved with this layout. The development of aluminum engines and new manufacturing processes has, however, made it possible to locate the engine at the rear without necessarily compromising stability.
Body
Automotive body designs are frequently categorized according to the number of doors, the arrangement of seats, and the roof structure. Automobile roofs are conventionally supported by pillars on each side of the body. Convertible models with retractable fabric tops rely on the pillar at the side of the windshield for upper body strength, as convertible mechanisms and glass areas are essentially nonstructural. Glass areas have been increased for improved visibility and for aesthetic reasons.
The high cost of new factory tools makes it impractical for manufacturers to produce totally new designs every year. Completely new designs usually have been programmed on three- to six-year cycles with generally minor refinements appearing during the cycle. In the past, as many as four years of planning and new tool purchasing were needed for a completely new design. Computer-aided design (CAD), testing by use of computer simulations, and computer-aided manufacturing (CAM) techniques may now be used to reduce this time requirement by 50 percent or more. See machine tool: Computer-aided design and computer-aided manufacturing (CAD/CAM).
Automotive bodies are generally formed out of sheet steel. The steel is alloyed with various elements to improve its ability to be formed into deeper depressions without wrinkling or tearing in manufacturing presses. Steel is used because of its general availability, low cost, and good workability. For certain applications, however, other materials, such as aluminum, fibreglass, and carbon-fibre reinforced plastic, are used because of their special properties. Polyamide, polyester, polystyrene, polypropylene, and ethylene plastics have been formulated for greater toughness, dent resistance, and resistance to brittle deformation. These materials are used for body panels. Tooling for plastic components generally costs less and requires less time to develop than that for steel components and therefore may be changed by designers at a lower cost.
To protect bodies from corrosive elements and to maintain their strength and appearance, special priming and painting processes are used. Bodies are first dipped in cleaning baths to remove oil and other foreign matter. They then go through a succession of dip and spray cycles. Enamel and acrylic lacquer are both in common use. Electrodeposition of the sprayed paint, a process in which the paint spray is given an electrostatic charge and then attracted to the surface by a high voltage, helps assure that an even coat is applied and that hard-to-reach areas are covered. Ovens with conveyor lines are used to speed the drying process in the factory. Galvanized steel with a protective zinc coating and corrosion-resistant stainless steel are used in body areas that are more likely to corrode.
Chassis
In most passenger cars through the middle of the 20th century, a pressed-steel frame—the vehicle’s chassis—formed a skeleton on which the engine, wheels, axle assemblies, transmission, steering mechanism, brakes, and suspension members were mounted. The body was flexibly bolted to the chassis during a manufacturing process typically referred to as body-on-frame construction. This process is used today for heavy-duty vehicles, such as trucks, which benefit from having a strong central frame, subjected to the forces involved in such activities as carrying freight, including the absorption of the movements of the engine and axle that is allowed by the combination of body and frame.
In modern passenger-car designs, the chassis frame and the body are combined into a single structural element. In this arrangement, called unit-body (or unibody) construction, the steel body shell is reinforced with braces that make it rigid enough to resist the forces that are applied to it. Separate frames or partial “stub” frames have been used for some cars to achieve better noise-isolation characteristics. The heavier-gauge steel present in modern component designs also tends to absorb energy during impacts and limit intrusion in accidents.
Engine
A wide range of engines has been used experimentally and in automotive production. The most successful for automobiles has been the gasoline-fueled reciprocating-piston internal-combustion engine, operating on a four-stroke cycle, while diesel engines are widely used for trucks and buses. The gasoline engine was originally selected for automobiles because it could operate more flexibly over a wide range of speeds, and the power developed for a given weight engine was reasonable; it could be produced by economical mass-production methods; and it used a readily available, moderately priced fuel. Reliability, compact size, exhaust emissions, and range of operation later became important factors.
There has been an ongoing reassessment of these priorities with new emphasis on the reduction of greenhouse gases (see greenhouse effect) or pollution-producing characteristics of automotive power systems. This has created new interest in alternate power sources and internal-combustion engine refinements that previously were not close to being economically feasible. Several limited-production battery-powered electric vehicles are marketed today. In the past they had not proved to be competitive, because of costs and operating characteristics. The gasoline engine, with new emission-control devices to improve emission performance, has been challenged in recent years by hybrid power systems that combine gasoline or diesel engines with battery systems and electric motors. Such designs are, however, more complex and therefore more costly.
The evolution of higher-performance engines in the United States led the industry away from long, straight engine cylinder layouts to compact six- and eight-cylinder V-type layouts for larger cars (with horsepower ratings up to about 350). Smaller cars depend on smaller four-cylinder engines. European automobile engines were of a much wider variety, ranging from 1 to 12 cylinders, with corresponding differences in overall size, weight, piston displacement, and cylinder bores. A majority of the models had four cylinders and horsepower ratings up to 120. Most engines had straight or in-line cylinders. There were, however, several V-type models and horizontally opposed two- and four-cylinder makes. Overhead camshafts were frequently employed. The smaller engines were commonly air-cooled and located at the rear of the vehicle; compression ratios were relatively low. Increased interest in improved fuel economy brought a return to smaller V-6 and four-cylinder layouts, with as many as five valves per cylinder to improve efficiency. Variable valve timing to improve performance and lower emissions has been achieved by manufacturers in all parts of the world. Electronic controls automatically select the better of two profiles on the same cam for higher efficiency when engine speeds and loads change.
Fuel
Specially formulated gasoline is essentially the only fuel used for automobile operation, although diesel fuels are used for many trucks and buses and a few automobiles, and compressed liquefied hydrogen has been used experimentally. The most important requirements of a fuel for automobile use are proper volatility, sufficient antiknock quality, and freedom from polluting by-products of combustion. The volatility is reformulated seasonally by refiners so that sufficient gasoline vaporizes, even in extremely cold weather, to permit easy engine starting. Antiknock quality is rated by the octane number of the gasoline. The octane number requirement of an automobile engine depends primarily on the compression ratio of the engine but is also affected by combustion-chamber design, the maintenance condition of engine systems, and chamber-wall deposits. In the 21st century regular gasoline carried an octane rating of 87 and high-test in the neighbourhood of 93.
Automobile manufacturers have lobbied for regulations that require the refinement of cleaner-burning gasolines, which permit emission-control devices to work at higher efficiencies. Such gasoline was first available at some service stations in California, and from 2017 the primary importers and refiners of gasoline throughout the United States were required to remove sulfur particles from fuel to an average level of 10 parts per million (ppm).
Vehicle fleets fueled by natural gas have been in operation for several years. Carbon monoxide and particulate emissions are reduced by 65 to 90 percent. Natural-gas fuel tanks must be four times larger than gasoline tanks for equivalent vehicles to have the same driving range. This compromises cargo capacity.
Ethanol (ethyl alcohol) is often blended with gasoline (15 parts to 85 parts) to raise its octane rating, which results in a smoother-running engine. Ethanol, however, has a lower energy density than gasoline, which results in decreased range per tankful.
Lubrication
All moving parts of an automobile require lubrication. Without it, friction would increase power consumption and damage the parts. The lubricant also serves as a coolant, a noise-reducing cushion, and a sealant between engine piston rings and cylinder walls. The engine lubrication system incorporates a gear-type pump that delivers filtered oil under pressure to a system of drilled passages leading to various bearings. Oil spray also lubricates the cams and valve lifters.
Wheel bearings and universal joints require a fairly stiff grease; other chassis joints require a soft grease that can be injected by pressure guns. Hydraulic transmissions require a special grade of light hydraulic fluid, and manually shifted transmissions use a heavier gear oil similar to that for rear axles to resist heavy loads on the gear teeth. Gears and bearings in lightly loaded components, such as generators and window regulators, are fabricated from self-lubricating plastic materials. Hydraulic fluid is also used in other vehicle systems in conjunction with small electric pumps and motors.
Cooling system
Almost all automobiles employ liquid cooling systems for their engines. A typical automotive cooling system comprises (1) a series of channels cast into the engine block and cylinder head, surrounding the combustion chambers with circulating water or other coolant to carry away excessive heat, (2) a radiator, consisting of many small tubes equipped with a honeycomb of fins to radiate heat rapidly, which receives and cools hot liquid from the engine, (3) a centrifugal-type water pump with which to circulate coolant, (4) a thermostat, which maintains constant temperature by automatically varying the amount of coolant passing into the radiator, and (5) a fan, which draws fresh air through the radiator.
For operation at temperatures below 0 °C (32 °F), it is necessary to prevent the coolant from freezing. This is usually done by adding some compound, such as ethylene glycol, to depress the freezing point of the coolant. By varying the amount of additive, it is possible to protect against freezing of the coolant down to any minimum temperature normally encountered. Coolants contain corrosion inhibitors designed to make it necessary to drain and refill the cooling system only every few years.
Air-cooled cylinders operate at higher, more efficient temperatures, and air cooling offers the important advantage of eliminating not only freezing and boiling of the coolant at temperature extremes but also corrosion damage to the cooling system. Control of engine temperature is more difficult, however, and high-temperature-resistant ceramic parts are required when design operating temperatures are significantly increased.
Pressurized cooling systems have been used to increase effective operating temperatures. Partially sealed systems using coolant reservoirs for coolant expansion if the engine overheats were introduced in the early 1970s. Specially formulated coolants that do not deteriorate over time eliminate the need for annual replacement.
Electrical system
The electrical system comprises a storage battery, generator, starting (cranking) motor, lighting system, ignition system, and various accessories and controls. Originally, the electrical system of the automobile was limited to the ignition equipment. With the advent of the electric starter on a 1912 Cadillac model, electric lights and horns began to replace the kerosene and acetylene lights and the bulb horns. Electrification was rapid and complete, and, by 1930, 6-volt systems were standard everywhere.
Increased engine speeds and higher cylinder pressures made it increasingly difficult to meet high ignition voltage requirements. The larger engines required higher cranking torque. Additional electrically operated features—such as radios, window regulators, and multispeed windshield wipers—also added to system requirements. To meet these needs, 12-volt systems replaced the 6-volt systems in the late 1950s around the world.
The ignition system provides the spark to ignite the air-fuel mixture in the cylinders of the engine. The system consists of the spark plugs, coil, distributor, and battery. In order to jump the gap between the electrodes of the spark plugs, the 12-volt potential of the electrical system must be stepped up to about 20,000 volts. This is done by a circuit that starts with the battery, one side of which is grounded on the chassis and leads through the ignition switch to the primary winding of the ignition coil and back to the ground through an interrupter switch. Interrupting the primary circuit induces a high voltage across the secondary terminal of the coil. The high-voltage secondary terminal of the coil leads to a distributor that acts as a rotary switch, alternately connecting the coil to each of the wires leading to the spark plugs.
Solid-state or transistorized ignition systems were introduced in the 1970s. These distributor systems provided increased durability by eliminating the frictional contacts between breaker points and distributor cams. The breaker point was replaced by a revolving magnetic-pulse generator in which alternating-current pulses trigger the high voltage needed for ignition by means of an amplifier electronic circuit. Changes in engine ignition timing are made by vacuum or electronic control unit (microprocessor) connections to the distributor.
The source of energy for the various electrical devices of the automobile is a generator, or alternator, that is belt-driven from the engine crankshaft. The design is usually an alternating-current type with built-in rectifiers and a voltage regulator to match the generator output to the electric load and also to the charging requirements of the battery, regardless of engine speed.
A lead-acid battery serves as a reservoir to store excess output of the generator. This provides energy for the starting motor and power for operating other electric devices when the engine is not running or when the generator speed is not sufficiently high for the load.
The starting motor drives a small spur gear so arranged that it automatically moves in to mesh with gear teeth on the rim of the flywheel as the starting-motor armature begins to turn. When the engine starts, the gear is disengaged, thus preventing damage to the starting motor from overspeeding. The starting motor is designed for high current consumption and delivers considerable power for its size for a limited time.
Headlights must satisfactorily illuminate the highway ahead of the automobile for driving at night or in inclement weather without temporarily blinding approaching drivers. This was achieved in modern cars with double-filament bulbs with a high and a low beam, called sealed-beam units. Introduced in 1940, these bulbs found widespread use following World War II. Such units could have only one filament at the focal point of the reflector. Because of the greater illumination required for high-speed driving with the high beam, the lower beam filament was placed off centre, with a resulting decrease in lighting effectiveness. Separate lamps for these functions can also be used to improve illumination effectiveness.
Dimming is automatically achieved on some cars by means of a photocell-controlled switch in the lamp circuit that is triggered by the lights of an oncoming car. Lamp clusters behind aerodynamic plastic covers permitted significant front-end drag reduction and improved fuel economy. In this arrangement, steerable headlights became possible with an electric motor to swivel the lamp assembly in response to steering wheel position. The regulations of various governments dictate brightness and field of view requirements for vehicle lights.
Signal lamps and other special-purpose lights have increased in usage since the 1960s. Amber-coloured front and red rear signal lights are flashed as a turn indication; all these lights are flashed simultaneously in the “flasher” (hazard) system for use when a car is parked along a roadway or is traveling at a low speed on a high-speed highway. Marker lights that are visible from the front, side, and rear also are widely required by law. Red-coloured rear signals are used to denote braking, and cornering lamps, in connection with turning, provide extra illumination in the direction of an intended turn. Backup lights provide illumination to the rear and warn anyone behind the vehicle when the driver is backing up. High-voltage light-emitting diodes (LEDs) have been developed for various signal and lighting applications.
Transmission
The gasoline engine must be disconnected from the driving wheels when it is started and when idling. This characteristic necessitates some type of unloading and engaging device to permit gradual application of load to the engine after it has been started. The torque, or turning effort, that the engine is capable of producing is low at low crankshaft speeds, increasing to a maximum at some fairly high speed representing the maximum, or rated, horsepower.
The efficiency of an automobile engine is highest when the load on the engine is high and the throttle is nearly wide open. At moderate speeds on level pavement, the power required to propel an automobile is only a fraction of this. Under normal driving conditions at constant moderate speed, the engine may operate at an uneconomically light load unless some means is provided to change its speed and power output.
The transmission is such a speed-changing device. Installed in the power train between the engine and the driving wheels, it permits the engine to operate at a higher speed when its full power is needed and to slow down to a more economical speed when less power is needed. Under some conditions, as in starting a stationary vehicle or in ascending steep grades, the torque of the engine is insufficient, and amplification is needed. Most devices employed to change the ratio of the speed of the engine to the speed of the driving wheels multiply the engine torque by the same factor by which the engine speed is increased.
The simplest automobile transmission is the sliding-spur gear type with three or more forward speeds and reverse. The desired gear ratio is selected by manipulating a shift lever that slides a spur gear into the proper position to engage the various gears. A clutch is required to engage and disengage gears during the selection process. The necessity of learning to operate a clutch is eliminated by an automatic transmission. Most automatic transmissions employ a hydraulic torque converter, a device for transmitting and amplifying the torque produced by the engine. Each type provides for manual selection of reverse and low ranges that either prevent automatic upshifts or employ lower gear ratios than are used in normal driving. Grade-retard provisions are also sometimes included to supply dynamic engine braking on hills. Automatic transmissions not only require little skill to operate but also make possible better performance than is obtainable with designs that require clutch actuation.
In hydraulic transmissions, shifting is done by a speed-sensitive governing device that changes the position of valves that control the flow of hydraulic fluid. The vehicle speeds at which shifts occur depend on the position of the accelerator pedal, and the driver can delay upshifts until higher speed is attained by depressing the accelerator pedal further. Control is by hydraulically engaged bands and multiple-disk clutches running in oil, either by the driver’s operation of the selector lever or by speed- and load-sensitive electronic control in the most recent designs. Compound planetary gear trains with multiple sun gears and planet pinions have been designed to provide a low forward speed, intermediate speeds, a reverse, and a means of locking into direct drive. This unit is used with various modifications in almost all hydraulic torque-converter transmissions. All transmission control units are interconnected with vehicle emission control systems that adjust engine timing and air-to-fuel ratios to reduce exhaust emissions.
Oil in the housing is accelerated outward by rotating vanes in the pump impeller and, reacting against vanes in the turbine impeller, forces them to rotate, as shown schematically in the figure. The oil then passes into the stator vanes, which redirect it to the pump. The stator serves as a reaction member providing more torque to turn the turbine than was originally applied to the pump impeller by the engine. Thus, it acts to multiply engine torque by a factor of up to 2 1/2 to 1.
Blades in all three elements are specially contoured for their specific function and to achieve particular multiplication characteristics. Through a clutch linkage, the stator is allowed gradually to accelerate until it reaches the speed of the pump impeller. During this period torque multiplication gradually drops to approach 1 to 1.
The hydraulic elements are combined with two or more planetary gear sets, which provide further torque multiplication between the turbine and the output shaft.
Continuously (or infinitely) variable transmissions provide a very efficient means of transferring engine power and, at the same time, automatically changing the effective input-to-output ratio to optimize economy by keeping the engine running within its best power range. Most designs employ two variable-diameter pulleys connected by either a steel or high-strength rubber V-belt. The pulleys are split so that effective diameters may be changed by an electrohydraulic actuator to change the transmission ratio. This permits the electronic control unit to select the optimum ratio possible for maximum fuel economy and minimum emissions at all engine speeds and loads. Originally these units were limited to small cars, but belt improvements have made them suitable for larger cars.
Additional Information
The four-wheeled transportation vehicle symbolizes the promise and the pitfalls of the modern age.
An automobile is a self-propelled motor vehicle intended for passenger transportation on land. It usually has four wheels and an internal combustion engine fueled most often by gasoline, a liquid petroleum product. Known more commonly as a car, formerly as a motorcar, it is one of the most universal of modern technologies, manufactured by one of the world’s largest industries. More than 73 million new automobiles were produced worldwide in the year 2017.
The scientific and technical building blocks of the automobile go back several hundred years. For example, in the late 1600s, Dutch scientist Christiaan Huygens invented a type of internal combustion engine sparked by gunpowder. The “horseless carriage” in its modern form had been developed by the end of the 19th century. At that time, it was not clear which of three fuel sources would become most commercially successful: steam, electric power, or gasoline. Cars run by steam engines could go at high speeds but had a short range and were inconvenient to start. Battery-powered electric cars had a 38 percent share of the United States automobile market in 1900, but they also had a limited range and recharging stations were hard to find.
The gasoline-powered automobile won the competition. By 1920, it had overtaken the streets and byways of Europe and the United States. The manufacturing methods introduced by U.S. carmaker Henry Ford revolutionized industrial manufacturing. Ford was the first to install assembly lines in his factory to speed up production. Such techniques reduced the price of Ford’s Model T until it became affordable for most middle-class families. As the 20th century progressed, modern life came to seem increasingly inconceivable, or at least highly inconvenient, without access to a car. Nowadays, the U.S. population drives more than 4.8 trillion kilometers (three trillion miles) every year on average.
But this fundamental component of industrial and consumer society has played a major role in destabilizing Earth’s atmosphere, on which all living things depend. The average automobile emits between four and nine tons (3,629 to 8,165 kilograms; 8,000 to 18,000 pounds) of carbon dioxide and other greenhouse gases per year. Every gallon of gasoline burned to operate a car emits just under 9.1 kilograms (20 pounds) of carbon dioxide. The transportation sector as a whole, including cars, trucks, trains, and aircraft, became the largest source of U.S. greenhouse gas emissions in 2017. Air pollution from automobile exhaust is also a major problem, as are car accidents, which killed more than 100 people per day in the United States in 2016, according to the National Highway Traffic Safety Administration.
:max_bytes(150000):strip_icc():format(webp)/GettyImages-1186091457-0c53b6749ceb49b79053f61f583eef03.jpg)
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2724 2026-03-16 00:04:16
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2523) Hematite
Gist
Hematite is a common iron oxide mineral and the world's most important iron ore, containing roughly 70% iron. It is recognized by its brilliant metallic gray to dull red color and characteristic reddish-brown streak, which is used for pigments and polishing. It is abundant on Earth and causes the red coloration on Mars.
Hematite occurs in a variety of igneous and metamorphic rocks, but is most abundant in sedimentary settings. In sedimentary rocks, hematite can either have formed from have originally formed directly from direct precipitation out of marine waters, or as a concentration and enrichment deposit formed from groundwater.
Summary
Hematite is a heavy and relatively hard oxide mineral, ferric oxide (Fe2O3), that constitutes the most important iron ore because of its high iron content (70 percent) and its abundance. Its name is derived from the Greek word for “blood,” in allusion to its red colour. Many of the various forms of hematite have separate names. The steel-gray crystals and coarse-grained varieties have a brilliant metallic lustre and are known as specular iron ore; thin scaly types are called micaceous hematite. Much hematite occurs in a soft, fine-grained, earthy form called red ochre or ruddle. Intermediate between these types are compact varieties, often with a reniform surface (kidney ore) or a fibrous structure (pencil ore). Red ochre is used as a paint pigment; a purified form, rouge, is used to polish plate glass.
The most important deposits of hematite are sedimentary in origin. The world’s largest production (nearly 75 million tons of hematite annually) comes from a sedimentary deposit in the Lake Superior district in North America. Other important deposits include those at Minas Gerais, Brazil (where the hematite occurs in metamorphosed sediments); Cerro Bolívar, Venezuela; and Labrador and Quebec, Canada. Hematite is found as an accessory mineral in many igneous rocks; commonly as a weathering product of siderite, magnetite, and other iron minerals; and almost universally as a pigmenting agent of sedimentary and other rocks. For detailed physical properties, see oxide mineral.
Details
Hematite is one of the most abundant minerals on Earth's surface and in the shallow crust. It is an iron oxide with a chemical composition of Fe2O3. It is a common rock-forming mineral found in sedimentary, metamorphic, and igneous rocks at locations throughout the world.
Hematite is the most important ore of iron. Although it was once mined at thousands of locations around the world, today almost all of the production comes from a few dozen large deposits where significant equipment investments allow companies to efficiently mine and process the ore. Most ore is now produced in China, Australia, Brazil, India, Russia, Ukraine, South Africa, Canada, Venezuela, and the United States.
Hematite has a wide variety of other uses, but their economic significance is very small compared to the importance of iron ore. The mineral is used to produce pigments, preparations for heavy media separation, radiation shielding, ballast, and many other products.
Physical Properties of Hematite
Hematite has an extremely variable appearance. Its luster can range from earthy to submetallic to metallic. Its color ranges include red to brown and black to gray to silver. It occurs in many forms that include micaceous, massive, crystalline, botryoidal, fibrous, oolitic, and others.
Even though hematite has a highly variable appearance, it always produces a reddish streak. Students in introductory geology courses are usually surprised to see a silver-colored mineral produce a reddish streak. They quickly learn that the reddish streak is the most important clue for identifying hematite.
Hematite is not magnetic and should not respond to a common magnet. However, many specimens of hematite contain enough magnetite that they are attracted to a common magnet. This can lead to an incorrect assumption that the specimen is magnetite or the weakly magnetic pyrrhotite. The investigator must check other properties to make a proper identification.
If the investigator checks the streak, a reddish streak will rule out identification as magnetite or pyrrhotite. Instead, if the specimen is magnetic and has a reddish streak, it is most likely a combination of hematite and magnetite.
Composition of Hematite
Pure hematite has a composition of about 70% iron and 30% oxygen by weight. Like most natural materials, it is rarely found with that pure composition. This is particularly true of the sedimentary deposits where hematite forms by inorganic or biological precipitation in a body of water.
Minor clastic sedimentation can add clay minerals to the iron oxide. Episodic sedimentation can cause the deposit to have alternating bands of iron oxide and shale. Silica in the form of jasper, chert, or chalcedony can be added by chemical, clastic, or biological processes in small amounts or in significant episodes. These layered deposits of hematite and shale or hematite and silica have become known as the "banded iron formations".
Geologic Occurrence
Hematite is found as a primary mineral and as an alteration product in igneous, metamorphic, and sedimentary rocks. It can crystallize during the differentiation of a magma or precipitate from hydrothermal fluids moving through a rock mass. It can also form during contact metamorphism when hot magmas react with adjacent rocks.
The most important hematite deposits formed in sedimentary environments. About 2.4 billion years ago, Earth’s oceans were rich in dissolved iron, but very little free oxygen was present in the water. Then a group of cyanobacteria became capable of photosynthesis. The bacteria used sunlight as an energy source to convert carbon dioxide and water into carbohydrates, oxygen, and water. This reaction released the first free oxygen into the ocean environment. The new oxygen immediately combined with the iron to form hematite, which sank to the bottom of the seafloor and became the rock units that we know today as the banded iron formations.
Soon, photosynthesis was occurring in many parts of Earth’s oceans, and extensive hematite deposits were accumulating on the seafloor. This deposition continued for hundreds of millions of years - from about 2.4 to 1.8 million years ago. This allowed the formation of iron deposits hundreds to several thousand feet thick that are laterally persistent over hundreds to thousands of square miles. They comprise some of the largest rock formations in Earth’s rock record.
Many of the sedimentary iron deposits contain both hematite and magnetite as well as other iron minerals. These are often in intimate association, and the ore is mined, crushed, and processed to recover both minerals. Historically, much of the hematite was not recovered and was sent to tailings piles. More efficient processing today allows more hematite to be recovered from the ore. The tailings can also be reprocessed to recover additional iron and reduce tailings volume.
Hematite on Mars?
NASA has discovered that hematite is one of the most abundant minerals in the rocks and soils on the surface of Mars. An abundance of hematite in Martian rocks and surface materials gives the landscape a reddish brown color and is why the planet appears red in the night sky. It is the origin of Mars' "Red Planet" nickname.
Uses of Hematite (Iron Ore)
Hematite is the world’s most important ore of iron. Although magnetite contains a higher percentage of iron and is easier to process, hematite is the leading ore because it is more abundant and present in deposits in many parts of the world.
Hematite is mined in some of the largest mines in the world. These mines require investments of billions of dollars, and some will remove over 100 million tons of ore per year. These open-pit mines can be hundreds to thousands of feet deep and several miles across by the time they have been worked to completion.
China, Australia, Brazil, India, Russia, Ukraine, South Africa, and the United States are the world’s leading producers of iron ore (includes hematite, magnetite, and other ores). Iron ore production in the United States occurs in Michigan and Minnesota.
Uses of Hematite (Pigment)
The name hematite is from the Greek word "haimatitis" which means "blood-red." That name stems from the color of hematite when it has been crushed to a fine powder. Primitive people discovered that hematite could be crushed and mixed with a liquid for use as a paint or cosmetic. Cave paintings, known as "pictographs," dating back to 40,000 years ago were created with hematite pigments.
Hematite continues to be one of the most important pigment minerals. It has been mined at many locations around the world and has been traded extensively as a red pigment. During the Renaissance when many painters began using oils and canvas, hematite was one of the most important pigments. Hematite color was opaque and permanent. It could be mixed with a white pigment to produce a variety of pink colors that were used to paint flesh.
Uses of Hematite (Gem Material)
Hematite is a minor gem material used to produce cabochons, beads, small sculptures, tumbled stones, and other items. The material used to manufacture these products is a silver-colored hematite with a solid, uniform texture. The bright silver color of hematite and its "weighty feel" make it a very popular tumbled stone.
Uses of Hematite (Healing Stone)
Some people believe that carrying pieces of tumble-polished hematite, known as "healing stones," will bring relief from certain medical problems. There is no scientific proof that this use of hematite has any positive effect beyond being a placebo. Using hematite as a "healing stone" or a "healing crystal" can actually be harmful because it diverts people from seeing a doctor who can provide proper care. Then when the person with the problem finally decides to see a doctor, their situation is more severe.
Other Uses of Hematite
Hematite is used for a number of other purposes. It is a very dense and inexpensive material that is effective at stopping x-rays. For that reason it is used for radiation shielding around medical and scientific equipment. The low cost and high density of hematite and other iron ores also makes them useful as ballast for ships.
Hematite can also be ground to a fine powder that when mixed with water will make a liquid with a very high specific gravity. These liquids are used in the "float-sink" processing of coal and other mineral material. The crushed coal, which has a very low specific gravity, is placed on the heavy liquid and the light clean coal floats, while high-specific-gravity impurities such as pyrite sink.
Finally, hematite is the material used to make polishing compounds known as "red rouge" and "jeweler's rouge." Red rouge is a hematite powder used to polish brass and other soft metals. It can be added to crushed corn cob media or crushed walnut shell media for tumble-polishing brass shell casings. Jeweler's rouge is a paste used on a soft cloth to polish gold and silver jewelry.
Additional Information
Hematite, also spelled as haematite, is a common iron oxide compound with the formula Fe2O3 and is widely found in rocks and soils. Hematite crystals belong to the rhombohedral lattice system which is designated the alpha polymorph of Fe2O3. It has the same crystal structure as corundum (Al2O3) and ilmenite (FeTiO3). With this crystal structure geometry it forms a complete solid solution at temperatures above 950 °C (1,740 °F).
Hematite occurs naturally in black to steel or silver-gray, brown to reddish-brown, or red colors. It is mined as an important ore mineral of iron. It is electrically conductive. Hematite varieties include kidney ore, martite (pseudomorphs after magnetite), iron rose and specularite (specular hematite). While these forms vary, they all have a rust-red streak. Hematite is not only harder than pure iron, but also much more brittle. The term kidney ore may be broadly used to describe botryoidal, mammillary, or reniform hematite.[8] Maghemite is a polymorph of hematite (γ-Fe2O3) with the same chemical formula, but with a spinel structure like magnetite.
Large deposits of hematite are found in banded iron formations. Gray hematite is typically found in places that have still, standing water, or mineral hot springs, such as those in Yellowstone National Park in North America. The mineral may precipitate in the water and collect in layers at the bottom of the lake, spring, or other standing water. Hematite can also occur in the absence of water, usually as the result of volcanic activity.
Clay-sized hematite crystals also may occur as a secondary mineral formed by weathering processes in soil, and along with other iron oxides or oxyhydroxides such as goethite, which is responsible for the red color of many tropical, ancient, or otherwise highly weathered soils.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#2725 2026-03-17 00:04:13
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,756
Re: Miscellany
2524) Microchip
Gist
Microchips (integrated circuits) are tiny silicon devices containing millions or billions of transistors that process, store, and manage data within electronics. They act as the "brains" or "nervous system" for devices ranging from smartphones and computers to cars, medical devices, and household appliances.
Microchips, also known as integrated circuits or computer chips, are the tiny, powerful devices at the heart of nearly every device we use today. These chips are essential building blocks in all modern technology: from smartphones and computers to cars and medical devices.
Summary
Microchips, those unassuming slivers of silicon, are more than just components; they are the linchpins of modern technology. Fundamentally, a microchip, or an integrated circuit, is a convergence of numerous electronic elements—transistors, resistors, capacitors—meticulously integrated onto a tiny silicon chip. This integration represents more than just a triumph in making things smaller; it stands as a powerful demonstration of human creativity and skill in the field of electronics.
The true value of microchips lies not in their physical form but in their pervasive influence across various technological domains. From the smartphone in your pocket to the satellites orbiting our planet, microchips are the unsung heroes, silently orchestrating the digital symphony that underpins our daily lives.
As we delve into the workings of microchips, this article aims to transcend the fleeting trends of the tech world, focusing instead on the enduring principles that make microchips a cornerstone of innovation. We'll explore their fundamental concepts, steering clear of ephemeral specifics, to appreciate their lasting impact on technology.
Details
A microchip is an electronic device made of a small, flat piece of semiconductor material modified with other dopants, oxides, and metals to create electronic components, including transistors, diodes, resistors, and capacitors connected in a circuit.
Microchips are also called:
* Integrated circuits (ICs)
* Computer chips
* Semiconductors
* Chips
Integrated circuits have replaced assemblies of discrete components attached by wires or printed circuit boards (PCBs) because they are a single monolithic device that is much smaller, uses much less power, and can be mass produced at a significantly lower cost.
Semiconductor materials were discovered in 1821 by Thomas Johann Seebeck, and the first working semiconductor transistors were created by Willam Shockley in 1947. The components and all their interconnects were then combined into a single device in 1959 by Robert Noyce. The key to this invention and all that followed was the planar manufacturing process, which used photolithography to deposit and remove materials one layer at a time in a precise manner.
Integrated circuits are an integral part of modern life, providing electronics for devices ranging from toys to deep space probes. In 2023, the worldwide revenue from microchip sales was $526.9 billion. That year’s sales also saw further growth in chip usage beyond computers: 32% were for communication, 17% for automotive applications, 14% for industrial devices, 11% for consumer electronics, and only 25% for computing.
Driven by Moore’s Law, which states that the number of transistors in an IC will double every two years, the growing complexity of the circuits and the ever-decreasing size of components make designing and manufacturing microchips more challenging with each generation of chips.
The general size of individual elements on a chip, referred to as feature size, is measured in nanometers (nm), or one-billionth of a meter. Current semiconductor manufacturers use 14-nm, 10-nm, 7-nm, 5-nm, and 3-nm processes, with 2-nm technologies coming online. For scale, a grain of rice is 5 million nanometers long.
In 2023, researchers created a record-breaking microprocessor containing 1.2 trillion transistors. Intel’s line of CPUs in 2024 include more than 100 million transistors on a single chip.
The Elements of a Typical Microchip
Integrated circuits are made from semiconductor material, usually silicon, stacked in overlapping layers. Here are the most common elements in a microchip:
* Silicon substrate: The base pure silicon crystal layer from which the other layers are constructed by removing or depositing other materials or doping the crystal material.
Silicon Wafer
* Layers: Electronic circuits are created on individual layers. Layers are modified with photolithography, etching, and deposition to produce the desired components and interconnections. Some layers also serve as electrical insulators.
* Vias: A conducting zone, usually cylindrical, used to transmit electrical signals between layers.
* Components: The electronic devices that make up the desired circuit. In most ICs, these consist of transistors, capacitors, diodes, resistors, and sometimes inductors.
* Interconnects: Metalized paths on a given layer that conduct electricity between components or to vias.
* Packaging: Once completed, the IC is placed inside an assembly called a semiconductor package that protects and insulates the delicate silicon chip, can connect multiple chips, and provides a way to connect the chip or chips to a larger electronics circuit.
How Microchips Are Manufactured
There are three steps to microchip manufacturing. Each step is highly optimized and automated to minimize cost, ensure quality, and maximize efficiency. Engineers designing ICs need to have a good understanding of the manufacturing process because each step determines the size, shape, and spacing of the components.
Step 1: Wafer Production
Making blank silicon wafers is the first step in semiconductor manufacturing. This process begins by growing a monocrystalline cylindrical ingot, called a boule, of semiconductor material, usually pure silicon. The boule is then sliced into a thin wafer, machined to create a flat surface, chemically etched to remove any damage from the machining, and polished. Electronic wafers are usually 100 to 450 mm in diameter. The most common size is 300 mm across and 755 µm thick.
Step 2: Fabrication
The circuitry, with all its components and interconnects, is created in a semiconductor fabrication facility, usually called a fab. Each layer and the topology of the circuitry is created in a series of highly controlled steps. Robots move wafers from machine to machine in clusters. Most chip fabrication processes follow these steps for each layer:
* Grow a silicon dioxide layer to cover the layer completely (also called passivation).
* Add a photoresist coating.
* Expose the photoresist layer to ultraviolet light in the pattern of the geometry you want to create. The photoresist layer is then developed, and the material exposed to light is removed. This is called photolithography.
* Use chemicals, usually a strong acid, to remove the oxide layer where the photoresist was removed. This is referred to as etching.
* Remove the undeveloped photoresist material.
* If doping is needed for the layer, ion implantation of contaminants into the crystal structure creates the desired semiconductor behavior for transistors and other components.
* For other materials, various forms of chemical or vapor deposition are used to create interconnects, vias, and other components.
Step 3: Packaging
Once each layer has been constructed and the wafer is cleaned and tested, it is cut into individual chips called dies. One or more dies are then attached to a structure through bonding, and the IC is encapsulated in different materials, depending on the application. Some packages contain a single chip, but the current trend is to combine multiple dies in a single package.
Microchip Types and Uses
The types and uses of integrated circuits are growing every year. Early ICs often performed a single function. But as the manufacturing technology and design tools have improved, chips have shifted to being multifunction.
Smartphones are a great example of how multiple types of chips can be combined in a single device for different uses. They contain radio frequency (RF) chips for the 5G radio and GPS, optoelectrical chips for the cameras, LED chips for the display, digital ICs for the processing units, micro-electromechanical systems (MEMS) chips for the accelerometer, and a dozen other integrated circuits to sense, control, and modify a vast number of uses.
The different types of chips can be categorized by the signaling they carry out.
Analog Integrated Circuits
Analog signals carry voltage across a continuous voltage range, not just a high or a low voltage signal. They are used to amplify, filter by frequency, and mix signals. The frequency and power of an analog IC can vary greatly, and higher frequencies and higher powers present significant design challenges.
Common uses for analog ICs include:
* Optical, thermal, and audio sensors
* Power management circuits
* Operational amplifiers (op-amps)
* Audio and video signal processing
* Telecommunications, including radio communication and optical signal processing
* RF circuits
* Signal conditioning
* Machine controllers
Digital Integrated Circuits
Digital ICs are logic devices that contain millions or billions of logic gates made of transistors. A signal running at a fixed clock frequency is modified or measured as either high or low, zero or one. By combining different logic devices, very complex calculations can be done with very little power used.
Some of the most common uses for digital ICs include:
* Logic ICs or processors
** Microprocessors
** Microcontrollers
** Application-specific integrated circuits (ASICs)
* Memory chips
* Field programmable gate arrays (FPGAs)
* Digital power management devices
* System-on-a-chip (SoC) devices
* Multi-die chips
Mixed-signal Integrated Circuits
Some integrated circuits combine circuitry to handle analog and digital signals and convert between the two to create mixed-signal integrated circuits. They are used when an analog signal is sensed or created and logical operations are needed to read, create, or modify that signal.
Some of the most common uses for mixed-signal ICs are:
* SoC devices
* Data acquisition chips
* RF CMOS circuits
* Clock/timing ICs
* Switched capacitor circuits
* Electro-optical devices
* MEMS devices
Future Trends in Microchip Technology
The future of microchips looks like the past, with more capabilities in smaller sizes while constantly driving the cost down. Advances in manufacturing will also create new opportunities for better performance and new applications.
Trends that will drive electrical engineering design and simulation in the near future include:
Shift to Fabless Design and Foundries
The industry has shifted over the years to a model where companies can design their own ICs and then outsource the manufacturing to a company that just makes chips. This is called fabless design, and the contract manufacturers are called foundries. This enables companies like Apple and Qualcomm to design innovative new products without the capital investment of building their own fabrication facilities. Engineers must design to the manufacturing processes and standards of the foundry they will use.
Smaller Feature Size
Feature sizes continue to shrink, creating power and signal integrity issues. To stay competitive, electrical engineers need to design using these new capabilities, as well as leveraging simulation and design best practices to avoid issues.
Electronic Device Complexity and Combined Functionality
With time, an increasing number of designers of electronic devices are looking for greater functionality in a single chip. Internet of Things (IoT) devices, new solid-state long-term storage, and GPU chips are examples of integrated circuits that will not only add new features and capabilities in the same chip, but the interaction between those functions will also become more sophisticated. Engineers need design and simulation tools to drive designs in which the industry is pulling the technology. Biomedical electronics like implanted microchips will be another area in which several capabilities are needed on a single chip.
Higher Clock Speeds and Frequencies
Increased performance demands and advances in RF technology are driving up clock speeds for digital ICs and frequencies for analog and mixed-signal chips. Both create issues with signal integrity and power management.
Greater Computer Power With Increased Energy Efficiency
The growth of data centers for high-performance computing to support trends like artificial intelligence, cryptocurrency mining, and IoT applications is driving demand for increased performance for microprocessors. These applications are pushing the industry for improvements in FPGAs, solid-state hard drives, memory, and GPUs, along with all the chips needed to connect everything at increasing data transfer speeds.
More Use Beyond Computing
The trend of increased microchip use in automotive, consumer electronics, and industrial applications will continue. Almost all products will be designed as smart devices with connectivity to broadband, sensors, and computing power — all of which need microchips.
Simulation in the Design of Microchips
The complexity and expense of microchip manufacturing make physically prototyping designs impractical. Instead, engineers use virtual prototyping through simulation to drive their design, verify the performance, and identify and solve problems before production begins. Simulation is also used to design packaging and optimize the semiconductor manufacturing machines that make the chips.
Using simulation for digital microchips begins with verifying the logical functionality of the digital design at an abstract level with RTL design. This includes a first look at power management with PowerArtist™ software. This tool can assess the power needs of a design early in the process and help drive a more power-efficient design.
Once the physical design is laid out, engineers can use RedHawk-SC™ software, the trusted industry leader for power noise and reliability for digital ICs, to assess voltage drop and electromigration in their designs.
On the analog and mixed-signal side of things, Totem™ software can be brought into the process for power integrity and reliability signoff. The industry’s trusted gold standard for electromigration multiphysics, it is certified by all major foundries down to 3 nm. It also works with PathFinder-SC™ software to calculate electrostatic discharge.
Once the design is optimized and verified, packaging engineers can use simulation to optimize the power, signal integrity, and robustness of the full microchip package. RedHawk-SC software is designed to handle large, multichip configurations, including system-in-package designs. Advanced semiconductor packaging uses 2.5D- and 3D-IC approaches to combine and connect multiple dies in the same package, and simulation with RedHawk-SC software is the primary way to verify and optimize the designs.
Once the electrical aspects of the design are resolved, packaging engineers can use tools like Mechanical™software and the Icepak® tool for structural reliability and thermal management.
Additional Information:
What is a microchip?
A microchip -- also called a chip, computer chip or integrated circuit (IC) -- is a unit of integrated circuitry that is manufactured at a microscopic scale using a semiconductor material, such as silicon or, to a lesser degree, germanium. Electronic components, such as transistors and resistors, are etched into the material in layers, along with intricate connections that link the components together and facilitate the flow of electric signals.
Microchip components are so small they're measured in nanometers (nm). Some components are now under 10 nm, making it possible to fit billions of components on a single chip. In 2021, IBM introduced a microchip based on 2 nm technology, smaller than the width of a strand of human DNA. A nanometer is one-billionth of a meter or one-millionth of a millimeter. At that scale, it is possible to fit up to 50 billion transistors on a microchip the size of a fingernail.
How are microchips made?
Microchip manufacturers rely on silicon for their chips because it is abundant, inexpensive and easy to work with. Also, it has proven to be a reliable semiconductor in a variety of devices. However, silicon might be reaching its practical limits as microchip technologies become smaller and more components are squeezed into the microchip in an effort to meet the ever-increasing demands for greater performance and more data. Researchers are actively working on a variety of solutions that they hope will be able to carry electronics into the future.
Microchips typically include the following types of components, which can number into the millions or even billions, depending on the type and function of the microchip:
* Transistors. Transistors are active components that control, generate or amplify electric signals within the circuitry, acting as a switch or gate. Multiple transistors can be combined into a single logic gate that compares input currents and produces a single output according to the specified logic.
* Resistors. Resistors are passive components that limit or regulate the flow of electrical current or that provide a specific voltage for an active device. Resistors control the electric signals that move between transistors.
* Capacitors. Capacitors are passive components that store electricity as an electrostatic field and release electric current. Capacitors are often used along with transistors in dynamic RAM (DRAM) to help maintain stored data.
* Diodes. Diodes are specialized components with two nodes that conduct electric current in one direction only. A diode can permit or block the flow of electric current and can be used for various roles, such as switches, rectifiers, voltage regulators or signal modulators.
What are the types of microchips?
Microchips drive all of today's electronics. Not only do these include computers, but also smartphones, network switches, home appliances, car and aircraft components, televisions and amplifiers, internet of things devices and countless other electronic systems. Microchips generally fall into one of the following two categories:
* Logic. This type of microchip does all the heavy lifting, processing the instructions and data that are fed to the device and subsequently to the chip in that device. The most common and widely used type of logic microchip is the central processing unit (CPU). However, this category also includes more specialized chips, such as graphical processing units (GPUs) and neural net processors.
* Memory. This type of microchip stores data. Data storage is either volatile or non-volatile. volatile memory chips require a constant source of power to retain their data. DRAM is a common example of a volatile memory chip. A non-volatile chip is one that can persist data even if the power supply is disrupted. A good example of non-volatile memory is NAND flash. Volatile memory devices tend to perform much better than non-volatile devices, although a number of efforts are underway to bridge the gap between the two, such as storage class memory.
Although many microchips focus on logic or memory only, other types of chips incorporate both, along with other capabilities. For example, system-on-a-chip (SoC) ICs are now widely used in devices such as smartphones and wearable technology and have begun making headway into the computer market, as evidenced by the Apple silicon series of chips. Another example is the application-specific IC, which can also include logic, memory and other capabilities, much like the SoC chip, except that the ASIC chip is customized for a specific purpose, such as medical equipment or an automotive component.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline