Math Is Fun Forum
You are not logged in.
- Topics: Active | Unanswered
#976 2021-03-31 00:07:03
- Jai Ganesh
- Administrator

- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
954) Vitiligo
Vitiligo, also called leukoderma, patchy loss of melanin pigment from the skin. Though the pigment-making cells of the skin, or melanocytes, are structurally intact, they have lost the ability to synthesize the pigment. The reason for this condition is unclear; research suggests that it may be an autoimmune condition.
Vitiligo appears clinically as milk-white irregularly oval patches of skin, which are small at the beginning but enlarge gradually. These patches are roughly symmetrical and are seen most commonly on the hands, wrists, face, neck, and upper trunk. The hair growing in the depigmented area is also white. Individuals with vitiligo (about 1 percent of the adult population) are usually in good general health, but vitiligo presents a cosmetic problem that can be serious in dark-skinned individuals. The normal skin colour rarely returns, and there is no known cure.
Vitiligo is a long-term skin condition characterized by patches of the skin losing their pigment. The patches of skin affected become white and usually have sharp margins. The hair from the skin may also become white. The inside of the mouth and nose may also be involved. Typically both sides of the body are affected. Often the patches begin on areas of skin that are exposed to the sun. It is more noticeable in people with dark skin. Vitiligo may result in psychological stress and those affected may be stigmatized.
The exact cause of vitiligo is unknown. It is believed to be due to genetic susceptibility that is triggered by an environmental factor such that an autoimmune disease occurs. This results in the destruction of skin pigment cells. Risk factors include a family history of the condition or other autoimmune diseases, such as hyperthyroidism, alopecia areata, and pernicious anemia. It is not contagious. Vitiligo is classified into two main types: segmental and non-segmental. Most cases are non-segmental, meaning they affect both sides; and in these cases, the affected area of the skin typically expands with time. About 10% of cases are segmental, meaning they mostly involve one side of the body; and in these cases, the affected area of the skin typically does not expand with time. Diagnosis can be confirmed by tissue biopsy.
There is no known cure for vitiligo. For those with light skin, sunscreen and makeup are all that is typically recommended. Other treatment options may include steroid creams or phototherapy to darken the light patches. Alternatively, efforts to lighten the unaffected skin, such as with hydroquinone, may be tried. Several surgical options are available for those who do not improve with other measures. A combination of treatments generally has better outcomes. Counselling to provide emotional support may be useful.
Globally about 1% of people are affected by vitiligo. In some populations it affects as many as 2–3%. Males and females are equally affected. About half show the disorder before age 20 and most develop it before age 40. Vitiligo has been described since ancient history.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#977 2021-04-01 00:13:54
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
955) Skin cancer
Skin cancer, disease characterized by the uncontrolled growth of cells in the skin. Skin cancers are of two distinct types: nonmelanoma and melanoma. Together they account for approximately half of all reported cancers. Melanomas are cancers of pigmented cells and are far more dangerous than nonmelanomas, which are the most common cancers in the United States. This article discusses nonmelanoma skin cancers.
Nonmelanomas are cancers of surface tissues (carcinomas). There are two forms of nonmelanoma, both of which can usually be cured with minor surgery. Squamous cell carcinomas develop from a layer of flat cells close to the skin’s surface and account for about one-fourth of nonmelanoma cases. Basal cell carcinomas account for roughly three-fourths of cases, and as many as 50 percent of patients with this form of the disease develop another skin cancer within five years of initial diagnosis. Basal cell carcinoma begins in a layer of cells underlying the squamous cells. The squamous and basal cell layers are both located in the epidermis.
Causes And Symptoms
Most cases of nonmelanoma skin cancer are caused by damage to DNA resulting from exposure to ultraviolet radiation of the sun. People with light complexions have a higher rate of skin cancer than those with dark skin, and males are more likely to develop skin cancer than females. Exposure to substances such as chemical As, coal, and tar has been linked to skin cancer, as has infection with human papillomavirus (HPV), particularly those infections causing genital warts. Other factors that increase skin cancer rates are chronic inflammatory skin diseases, long-term treatment for psoriasis, previous radiation treatment, and immune suppression. The rare congenital disorders xeroderma pigmentosum and basal cell nevus are also associated with increased risk.
The predominant symptom of nonmelanoma skin cancer is an unusual growth, mole, or other abnormal appearance on the skin. Abnormalities may be raised or flat and may be red, pink, black, blue, brown, or flesh-coloured. Moles or growths that are new, that grow or change shape rapidly, or that will not heal are particular signs of skin cancer and should be examined by a dermatologist.
Diagnosis And Prognosis
If cancer is suspected, a diagnosis is made following a skin biopsy. Depending on the severity of the skin lesion, a biopsy can be conducted by scraping surface cells, by using a narrow punch to extract a larger tissue sample, or by excising a section of skin and surrounding tissue with a scalpel.
Once nonmelanoma skin cancer has been diagnosed, its stage is determined to indicate how far the cancer has progressed. Stage 0 skin cancer is also called squamous cell carcinoma in situ, or Bowen disease, and is confined to the epidermis. Stage I cancers are 2 cm (approximately 3/4 inch) or less in size; stage II, more than 2 cm. Neither has spread beyond the skin. Stage III cancers have spread to deeper layers of the skin, underlying tissues, or nearby lymph nodes. Stage IV cancers have spread to other parts of the body such as the muscles, bones, lungs, nerves, or brain.
Very few cases of nonmelanoma spread to other tissues before they are detected and removed. Basal cell carcinomas rarely spread to surrounding tissues, and five-year survival rates approach 100 percent when these cancers are detected early, as most are. A small percentage of basal cell carcinomas spread to nearby lymph nodes and surrounding tissues; the five-year survival rate in these cases is very low. Squamous cell carcinomas also have an extremely high five-year survival rate when detected early, but the rate drops considerably if the cancer has spread.
Treatment
If diagnosed early, nonmelanoma skin cancers can be cured with minor surgery to remove the affected tissue. Removal may be accomplished by a simple surgical excision, by freezing the cells with liquid nitrogen, or by destroying them with a laser. In some superficial cancers the cells may be removed by merely scraping them off; any residual cancer cells are then killed with pulses of electricity. A procedure known as Moh surgery shaves off cells one layer at a time, stopping when microscopic analysis indicates that no cancer remains. In some cases, removal of nearby lymph nodes may also be necessary.
Radiation therapy can be used to cure very small cancers or to delay progression of larger cancers. It is sometimes used in conjunction with surgery to kill any cancer cells left behind. Side effects of radiation treatment may include vomiting, diarrhea, fatigue, or skin irritation resembling a sunburn or suntan.
Chemotherapy is sometimes used to treat skin cancers by directly applying a chemotherapeutic agent to the affected tissue; this reduces side effects, which can resemble those of radiation treatment. In the rare cases when nonmelanoma has spread to distant tissues, systemic chemotherapy may be necessary, although it generally will not cure the cancer.
Prevention
Skin cancer can be prevented by avoiding risk factors, particularly exposure to ultraviolet radiation from the sun. Sunlamps and tanning beds should be avoided, and the skin should be protected with sunscreen or clothing when outdoors. Some medical societies recommend a skin examination by a physician every three years for people between the ages of 20 and 40 and yearly examinations thereafter. Regular self-examinations of the skin are also recommended, and any unusual growth or appearance should be checked by a physician.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#978 2021-04-02 00:04:36
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
956) Tear duct and glands
Tear duct and glands, also called lachrymal, or lacrimal, duct and glands, structures that produce and distribute the watery component of the tear film. Tears consist of a complex and usually clear fluid that is diffused between the eye and the eyelid. Further components of the tear film include an inner mucous layer produced by specialized conjunctival cells and an outer lipid layer produced by meibomian glands along the eyelid margin. The mucous layer helps the tear film adhere to the eye surface, while the lipid layer serves to reduce tear evaporation. Tears prevent excessive drying of the surfaces of the eye (such as the conjunctiva and cornea), provide some nutrition and oxygen to surface structures, and possess antibacterial properties.
Tears are constantly secreted at a relatively regular rate from satellite (or accessory) lacrimal glands located high in the superior upper lid. Reflex tearing, such as that stimulated by eye irritation, bright lights, or emotional upset, is provided by the main lacrimal glands. Each main lacrimal gland lies in a hollow space in the inner surfaces of the frontal bone, located above and laterally to the eye. Each is about the size and shape of a shelled almond and is divided by a fibrous partition into an upper and a lower portion. Ducts from the gland discharge the tears onto the eye surface through openings, where the conjunctiva lining the upper lid meets the conjunctiva that covers the eyeball (an area called the fornix). Tears leave each eye by way of upper and lower canalicular ducts, which have barely visible openings, called puncta, at the nasal end of the upper and lower lid margins. The canaliculi lead to the lacrimal sac near the inner corner of each eye, which itself empties into the nasolacrimal duct, a tubelike structure that directs tears into the nasal cavity.
Diseases that damage the lacrimal gland, and thus decrease tear secretion, can lead to chronic dry eye, which ultimately can threaten vision. Treatment of chronic dry eye consists of artificial lubrication and, in some cases, mechanical closure of the puncta or surgery to partially close the lids.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#979 2021-04-03 00:19:43
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
957) Flash point
Flash point, the lowest temperature at which a liquid (usually a petroleum product) will form a vapour in the air near its surface that will “flash,” or briefly ignite, on exposure to an open flame. The flash point is a general indication of the flammability or combustibility of a liquid. Below the flash point, insufficient vapour is available to support combustion. At some temperature above the flash point, the liquid will produce enough vapour to support combustion. (This temperature is known as the fire point.)
The use of the flash point as a measure of a liquid’s hazardousness dates from the 19th century. Before gasoline became important, kerosene was the main petroleum product (used mainly as fuel for lamps and stoves), and there was a tendency on the part of petroleum distillers to leave as much as possible of the commercially worthless gasoline in the kerosene in order to sell more product. This adulteration of kerosene with highly volatile gasoline caused numerous fires and explosions in storage tanks and oil lamps. Legal measures were instituted to curb the danger, and test methods were prescribed and minimum flash points set.
Flash points are measured by heating a liquid to specific temperatures under controlled conditions and then applying a flame. The test is done in either an “open cup” or a “closed cup” apparatus, or in both, in order to mimic the conditions of storage and the workplace. Representative liquids and their approximate flash points are:
• automotive gasoline, −43 °C (−45 °F)
• ethyl alcohol, 13 °C (55 °F)
• automotive diesel fuel, 38 °C (100 °F)
• kerosene, 42–72 °C (108–162 °F)
• home heating oil, 52–96 °C (126–205 °F)
• SAE 10W-30 motor oil, 216 °C (421 °F)
Commercial products must adhere to specific flash points that have been set by regulating authorities.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#980 2021-04-04 00:10:02
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
958) Fire
Fire, rapid burning of combustible material with the evolution of heat and usually accompanied by flame. It is one of the human race’s essential tools, control of which helped start it on the path toward civilization.
The original source of fire undoubtedly was lightning, and such fortuitously ignited blazes remained the only source of fire for aeons. For some years Peking man, about 500,000 BCE, was believed to be the earliest unquestionable user of fire; evidence uncovered in Kenya in 1981 and in South Africa in 1988, however, suggests that the earliest controlled use of fire by hominids dates from about 1,420,000 years ago. Not until about 7000 BCE did Neolithic man acquire reliable fire-making techniques, in the form either of drills, saws, and other friction-producing implements or of flint struck against pyrites. Even then it was more convenient to keep a fire alive permanently than to reignite it.
Original Uses Of Fire
The first human beings to control fire gradually learned its many uses. Not only did they use fire to keep warm and cook their food; they also learned to use it in fire drives in hunting or warfare, to kill insects, to obtain berries, and to clear forests of underbrush so that game could be better seen and hunted. Eventually they learned that the burning of brush produced better grasslands and therefore more game.
With the achievement of agriculture in Neolithic times in the Middle East about 7000 BCE, there came a new urgency to clear brush and trees. The first agriculturists made use of fire to clear fields and to produce ash to serve as fertilizer. This practice, called slash-and-burn cultivation, persists in many tropical areas and some temperate zones today.
Manufacture Of Fire
The step from the control of fire to its manufacture is great and required hundreds of thousands of years. The number and variety of inventions of such manufacture are difficult to imagine. Not until Neolithic times is there evidence that human beings actually knew how to produce fire. Whether a chance spark from striking flint against pyrites or a spark made by friction while drilling a hole in wood gave human beings the idea for producing fire is not known; but flint and pyrites, as well as fire drills, have been recovered from Neolithic sites in Europe.
Most widespread among prehistoric and later primitive peoples is the friction method of producing fire. The simple fire drill, a pointed stick of hard wood twirled between the palms and pressed into a hole on the edge of a stick of softer wood, is almost universal. The fire-plow and the fire saw are variations on the friction method common in Oceania, Australia, and Indonesia. Mechanical fire drills were developed by the Eskimo, ancient Egyptians, Asian peoples, and a few American natives. A fire piston that produced heat and fire by the compression of air in a small tube of bamboo was a complex device invented and used in southeastern Asia, Indonesia, and the Philippines. About 1800 a metal fire piston was independently invented in Europe. In 1827 the English chemist John Walker invented the friction match containing phosphorous sulfate, essentially the same as that which is in use today.
Fire In Religion And Philosophy
The sacred fires and fire drills of religious rituals and the numerous fire-gods of world mythology must be interpreted as additional evidence of both the antiquity and the importance of fire in human history. In the ancient Vedic scriptures, Agni, or Fire, is the messenger between the people and their gods and the personification of the sacrificial fire. Brahman households today are supposed to maintain a sacred fire for the worship of Agni, much as the ancient Romans kept a holy perpetual fire cared for by the vestal virgins and as the Greeks tended and transported the sacred fire of Hestia during migrations. The Zoroastrians of Iran placed fire at the centre of their religion and worshiped it as the most subtle and ethereal principle and the most potent and sacred power, thought to have been presented to man directly from heaven and kindled by the Deity himself. Among the Israelites, Abraham might be viewed as a reformer who resisted the ancient worship of Moloch, the god of fire, by child sacrifice. In Siberia both the primitive Koryak and Chuckchi and the more civilized Buryat honoured the fire-god by keeping all filth and impurities away from their fires and hearths. The need to protect fire from contamination was also a belief in parts of Africa, North and South America, and elsewhere. The Aztec of Mexico and the Inca of Peru worshiped gods of fire with sacred flames, which the Inca ignited by concentrating the Sun’s rays with a concave metallic mirror.
The great Greek scientists and philosophers found fire just as significant as did the mystics of religion. Aristotle, for example, declared fire, along with water, earth, and air, to be one of the four general and essential elements of life and of all things. Plato asserted that God used the four elements in the creation of the world. Heraclitus attributed to fire the essential force for creation.
Fire And The Growth Of Civilization
Familiarity with fire, resulting from its easy production by flint and steel, phosphorus matches, or electricity, has led modern civilizations to take fire for granted. Yet, just as the initial control of fire was essential to the development of human beings from Old Stone Age hunters of the tropical forests into the first village-dwelling farmers of the Neolithic, so fire has been essential at every stage of the growth of civilization during the succeeding 10,000 years. From the use of fire to cook food, to clear land, and to furnish warmth and illumination in caves or hovels, fire has been applied to vessels of clay to make pottery and to pieces of ore to obtain copper and tin, to combine these to make bronze (c. 3000 BCE), and to obtain iron (c. 1000 BCE). Much of the modern history of technology and science might be characterized as a continual increase in the amount of energy available through fire and brought under human control. Most of the increased available energy has come from ever greater amounts and kinds of fires.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#981 2021-04-05 00:25:38
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
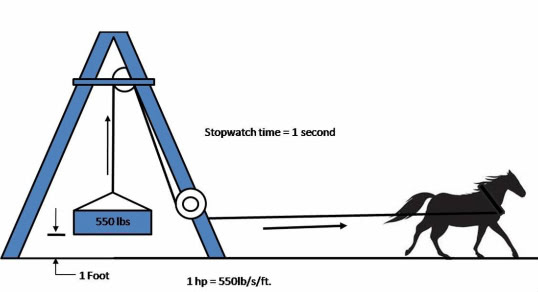
959) Horsepower
Horsepower, the common unit of power; i.e., the rate at which work is done. In the British Imperial System, one horsepower equals 33,000 foot-pounds of work per minute—that is, the power necessary to lift a total mass of 33,000 pounds one foot in one minute. This value was adopted by the Scottish engineer James Watt in the late 18th century, after experiments with strong dray horses, and is actually about 50 percent more than the rate that an average horse can sustain for a working day. The electrical equivalent of one horsepower is 746 watts in the International System of Units (SI), and the heat equivalent is 2,545 BTU (British Thermal Units) per hour. Another unit of power is the metric horsepower, which equals 4,500 kilogram-metres per minute (32,549 foot-pounds per minute), or 0.9863 horsepower.
Horsepower at the output shaft of an engine, turbine, or motor is termed brake horsepower or shaft horsepower, depending on what kind of instrument is used to measure it. Horsepower of reciprocating engines, particularly in the larger sizes, is often expressed as indicated horsepower, which is determined from the pressure in the cylinders. Brake or shaft horsepower is less than indicated horsepower by the amount of power lost to friction within the engine itself, which may amount to 10 percent or more of the indicated horsepower. Electric motor horsepower can be determined from the electrical input in watts, allowing for heat and friction losses in the motor itself. Thrust horsepower of jet engines and rockets is equal to the thrust in pounds force times the speed of the vehicle in miles per hour divided by 375 (which is equal to one horsepower measured in mile-pounds per hour).
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#982 2021-04-06 00:09:57
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
960) Week
Week, period of seven days, a unit of time artificially devised with no astronomical basis. The week’s origin is generally associated with the ancient Jews and the biblical account of the Creation, according to which God laboured for six days and rested on the seventh. Evidence indicates, however, that the Jews may have borrowed the idea of the week from Mesopotamia, for the Sumerians and the Babylonians divided the year into weeks of seven days each, one of which they designated a day of recreation.
The Babylonians named each of the days after one of the five planetary bodies known to them (Mercury, Venus, Mars, Jupiter, and Saturn) and after the Sun and the Moon, a custom later adopted by the Romans. For centuries the Romans used a period of eight days in civil practice, but in 321 CE Emperor Constantine established the seven-day week in the Roman calendar and designated Sunday as the first day of the week. Subsequent days bore the names Moon’s-day, Mars’s-day, Mercury’s-day, Jupiter’s-day, Venus’s-day, and Saturn’s-day. Constantine, a convert to Christianity, decreed that Sunday should be a day of rest and worship.
The days assigned by the Romans to the Sun, Moon, and Saturn were retained for the corresponding days of the week in English (Sunday, Monday, and Saturday) and several related languages. The Roman names for the other days of the week were retained in Romance languages. (For example, Friday, Venus’s-day is viernes in Spanish and vendredi in French.) The other weekday names in English are derived from Anglo-Saxon words for the gods of Teutonic mythology. Tuesday comes from Tiu, or Tiw, the Anglo-Saxon name for Tyr, the Norse god of war. Tyr was one of the sons of Odin, or Woden, the supreme deity after whom Wednesday was named. Similarly, Thursday originates from Thor’s-day, named in honour of Thor, the god of thunder. Friday was derived from Frigg’s-day, Frigg, the wife of Odin, representing love and beauty, in Norse mythology.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#983 2021-04-07 00:19:17
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
961) Pascal
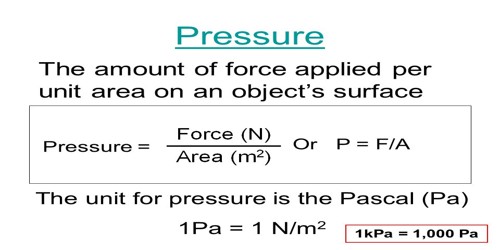
Pascal (Pa), unit of pressure and stress in the metre-kilogram-second system (the International System of Units [SI]). It was named in honour of the French mathematician-physicist Blaise Pascal (1623–62). A pascal is a pressure of one newton per square metre, or, in SI base units, one kilogram per metre per second squared. This unit is inconveniently small for many purposes, and the kilopascal (kPa) of 1,000 newtons per square metre is more commonly used. For example, standard atmospheric pressure (or 1 atm) is defined as 101.325 kPa. The millibar, a unit of air pressure often used in meteorology, is equal to 100 Pa. (For comparison, one pound per square inch equals 6.895 kPa.)
Pressure, in the physical sciences, the perpendicular force per unit area, or the stress at a point within a confined fluid. The pressure exerted on a floor by a 42-pound box the bottom of which has an area of 84 square inches is equal to the force divided by the area over which it is exerted; i.e., it is one-half pound per square inch. The weight of the atmosphere pushing down on each unit area of Earth’s surface constitutes atmospheric pressure, which at sea level is about 15 pounds per square inch. In SI units, pressure is measured in pascals; one pascal equals one newton per square metre. Atmospheric pressure is close to 100,000 pascals.
The pressure exerted by a confined gas results from the average effect of the forces produced on the container walls by the rapid and continual bombardment of the huge number of gas molecules. Absolute pressure of a gas or liquid is the total pressure it exerts, including the effect of atmospheric pressure. An absolute pressure of zero corresponds to empty space or a complete vacuum.
Measurement of pressures by ordinary gauges on Earth, such as a tire-pressure gauge, expresses pressure in excess of atmospheric. Thus, a tire gauge may indicate a pressure of 30 pounds (per square inch), the gauge pressure. The absolute pressure exerted by the air within the tire, including atmospheric pressure, is 45 pounds per square inch. Pressures less than atmospheric are negative gauge pressures that correspond to partial vacuums.
Hydrostatic pressure is the stress, or pressure, exerted equally in all directions at points within a confined fluid (liquid or gas). It is the only stress possible in a fluid at rest.
Lithostatic pressure, the stress exerted on a body of rock by surrounding rock, is a pressure in Earth’s crust somewhat analogous to hydrostatic pressure in fluids. Lithostatic pressure increases with depth below Earth’s surface.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#984 2021-04-08 00:17:21
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
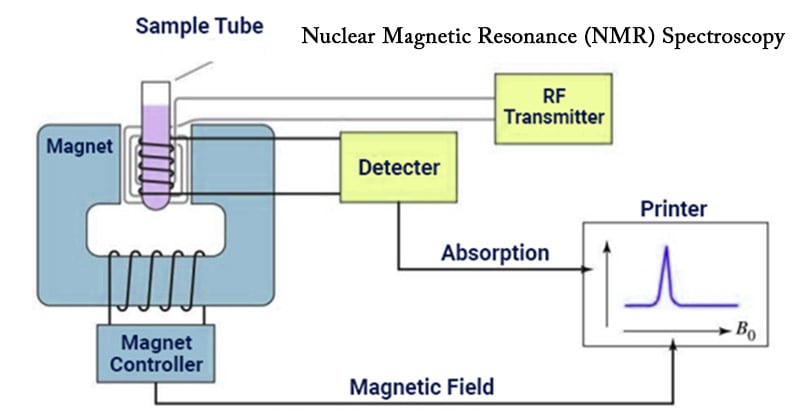
962) Nuclear magnetic resonance
Nuclear magnetic resonance (NMR), selective absorption of very high-frequency radio waves by certain atomic nuclei that are subjected to an appropriately strong stationary magnetic field. This phenomenon was first observed in 1946 by the physicists Felix Bloch and Edward M. Purcell independently of each other. Nuclei in which at least one proton or one neutron is unpaired act like tiny magnets, and a strong magnetic field exerts a force that causes them to precess in somewhat the same way that the axes of spinning tops trace out cone-shaped surfaces while they precess in the Earth’s gravitational field. When the natural frequency of the precessing nuclear magnets corresponds to the frequency of a weak external radio wave striking the material, energy is absorbed from the radio wave. This selective absorption, called resonance, may be produced either by tuning the natural frequency of the nuclear magnets to that of a weak radio wave of fixed frequency or by tuning the frequency of the weak radio wave to that of the nuclear magnets (determined by the strong constant external magnetic field).
Nuclear magnetic resonance is used to measure nuclear magnetic moments, the characteristic magnetic behaviour of specific nuclei. Because these values are significantly modified by the immediate chemical environment, however, NMR measurements provide information about the molecular structure of various solids and liquids.
By the early 1980s nuclear magnetic resonance techniques had begun to be used in medicine to visualize soft tissues of the body. This application of NMR, called magnetic resonance imaging (MRI), presented a hazard-free, noninvasive way to generate visual images of thin slices of the body by measuring the nuclear magnetic moments of ordinary hydrogen nuclei in the body’s water and lipids (fats). NMR images show great sensitivity in differentiating between normal tissues and diseased or damaged ones. By the late 1980s MRI had proved superior to most other imaging techniques in providing images of the brain, heart, liver, kidneys, spleen, pancreas, breast, and other organs. MRI provides relatively high-contrast, variable-toned images that can show tumours, blood-starved tissues, and neural plaques resulting from multiple sclerosis. The technique presents no known health hazards, but it cannot be used on individuals who have cardiac pacemakers or certain other metal-containing devices implanted in their bodies.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#985 2021-04-09 00:18:16
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
963) Horticulture
Horticulture, the branch of plant agriculture dealing with garden crops, generally fruits, vegetables, and ornamental plants. The word is derived from the Latin hortus, “garden,” and colere, “to cultivate.” As a general term, it covers all forms of garden management, but in ordinary use it refers to intensive commercial production. In terms of scale, horticulture falls between domestic gardening and field agriculture, though all forms of cultivation naturally have close links.
Horticulture is divided into the cultivation of plants for food (pomology and olericulture) and plants for ornament (floriculture and landscape horticulture). Pomology deals with fruit and nut crops. Olericulture deals with herbaceous plants for the kitchen, including, for example, carrots (edible root), asparagus (edible stem), lettuce (edible leaf), cauliflower (edible flower buds), tomatoes (edible fruit), and peas (edible seed). Floriculture deals with the production of flowers and ornamental plants; generally, cut flowers, pot plants, and greenery. Landscape horticulture is a broad category that includes plants for the landscape, including lawn turf but particularly nursery crops such as shrubs, trees, and vines.
The specialization of the horticulturist and the success of the crop are influenced by many factors. Among these are climate, terrain, and other regional variations.
Horticultural Regions
Temperate zones
Temperate zones for horticulture cannot be defined exactly by lines of latitude or longitude but are usually regarded as including those areas where frost in winter occurs, even though rarely. Thus, most parts of Europe, North America, and northern Asia are included, though some parts of the United States, such as southern Florida, are considered subtropical. A few parts of the north coast of the Mediterranean and the Mediterranean islands are also subtropical. In the Southern Hemisphere, practically all of New Zealand, a few parts of Australia, and the southern part of South America have temperate climates. For horticultural purposes altitude is also a factor; the lower slopes of great mountain ranges, such as the Himalayas and the Andes, are included. Thus, the temperate zones are very wide and the range of plants that can be grown in them is enormous, probably greater than in either the subtropical or tropical zones. In the temperate zones are the great coniferous and deciduous forests: pine, spruce, fir, most of the cypresses, the deciduous oaks (but excluding many of the evergreen ones), ash, birch, and linden.
The temperate zones are also the areas of the grasses—the finest lawns particularly are in the regions of moderate or high rainfall—and of the great cereal crops. Rice is excluded as being tropical, but wheat, barley, corn (maize), and rye grow well in the temperate zones.
Plants in the temperate zones benefit from a winter resting season, which clearly differentiates them from tropical plants, which tend to grow continuously. Bulbs, annuals, herbaceous perennials, and deciduous trees become more frost-resistant with the fall of sap and therefore have a better chance of passing the resting season undamaged. Another influence is the varying length of darkness and light throughout the year, so that many plants, such as chrysanthemums, have a strong photoperiodism. The chrysanthemum flowers only in short daylight periods, although artificial lighting in nurseries can produce flowers the year round.
Most of the great gardens of the world have been developed in temperate zones. Particular features such as rose gardens, herbaceous borders, annual borders, woodland gardens, and rock gardens are also those of temperate-zone gardens. Nearly all depend for their success on the winter resting period.
Tropical zones
There is no sharp line of demarcation between the tropics and the subtropics. Just as many tropical plants can be cultivated in the subtropics, so also many subtropical and even temperate plants can be grown satisfactorily in the tropics. Elevation is a determining factor. For example, the scarlet runner bean, a common plant in temperate regions, grows, flowers, and develops pods normally on the high slopes of Mount Meru in Africa near the Equator, but it will not set pods in Hong Kong, a subtropical situation a little south of the Tropic of Cancer but at a low elevation.
In addition to elevation, another determinant is the annual distribution of rainfall. Plants that grow and flower in the monsoon areas, as in India, will not succeed where the climate is uniformly wet, as in Bougainville in the Solomon Islands. Another factor is the length of day, the number of hours the Sun is above the horizon; some plants flower only if the day is long, but others make their growth during the long days and flower when the day is short. Certain strains of the cosmos plant are so sensitive to light that where the day is always about 12 hours, as near the Equator, they flower when only a few inches high; if grown near the Tropic of Cancer or the Tropic of Capricorn, they attain a height of several feet, if the seeds are sown in the spring, before flowering in the short days of autumn and winter. Poinsettia is a short-day plant that may be seen in flower in Singapore on any day of the year, while in Trinidad it is a blaze of glory only in late December.
In the tropics of Asia and parts of Central and South America, the dominant features of the gardens are flowering trees, shrubs, and climbers. Herbaceous plants are relatively few, but many kinds of orchids can be grown.
Vegetable crops vary in kind and quality with the presence or absence of periodic dry seasons. In the uniformly wet tropics, the choice is limited to a few root crops and still fewer greens. Sweet potatoes grow and bear good crops where the average monthly rainfall, throughout the year, exceeds 25 cm (10 inches), but they grow even better where there is a dry season. The same can be said of taro, yams, and cassava. Tropical greens from the Malay Peninsula are not as good as those grown in South China, the Hawaiian Islands, and Puerto Rico. They include several spinaches, of which Chinese spinach or amaranth is the best; several cabbages; Chinese onions and chives; and several gourds, cucumbers, and, where there is a dry season, watermelons. Eggplants, peppers, and okra are widely cultivated. Many kinds of beans can be grown successfully, including the French bean from the American subtropics, the many varieties of the African cowpea, and yard-long bean. The yam bean, a native of tropical America, is grown for its edible tuber. In the drier areas the pigeon pea, the soybean, the peanut (groundnut), and the Tientsin green bean are important crops. Miscellaneous crops include watercress, ginger, lotus, and bamboo.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#986 2021-04-10 00:16:47
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
964) Dermatology
Summary : What is dermatology?
Dermatology is a branch of medicine that deals with the skin and diseases of the skin. It concerns the study, research and diagnosis of normal skin and disorders of the skin. Cancers, cosmetic and aging conditions of the skin, fat, hair, nails and oral and genital membranes are all aspects of dermatology.
Subspecialties of the dermatology field include dermatopathology, which is involved with the pathology of the skin; immunodermatology, which specializes in the treatment of immune-mediated skin disorders, including lupus, bullous pemphigoid and pemphigus vulgaris; Mohs’ surgery, which involves removing tumors from the skin without harming healthy cells; and pediatric dermatology, in which dermatologists may treat infants, hereditary skin disorders and children.
An expert in the field of dermatology is a dermatologist. A dermatologist may be involved with medical or surgical treatments. Dermatologists may perform a range of procedures, many of which are cosmetic. These include cosmetic filler injections, hair removal or transplantation, intralesional treatment, laser therapy, photodynamic therapy, phototherapy, tattoo removal, tumescent liposuction, radiation therapy and vitiligo surgery.
Other treatments in the dermatology field include cryosurgery, which is the treatment of warts, skin cancers or other dermatoses; allergy testing; systemic therapies such as antibiotics, immunomodulators or injectable products; or topical therapies.
The skin is the largest organ in the body. Moreover, because the entire surface area of the skin is visible, dermatologists have the advantage of direct visual examination.
Details : A dermatologist is a doctor that specializes in treating skin, hair, nail, and mucous membrane disorders and diseases.
They can also address cosmetic issues, helping to revitalize the appearance of the skin, hair, and nails.
The Centers for Disease Control and Prevention (CDC) estimate that, in the United States, there were 39 million visits to office-based dermatologists, who were not federally employed, in 2010.
Below, we explore common issues that dermatologists encounter, the treatments they offer, and the qualifications involved.
What is dermatology?
Dermatology is an area of medicine that focuses on health issues affecting the skin, hair, nails, and mucous membranes.
The skin is the largest organ of the body. It is also the first line of defense against pathogens and injury, and it can be a good indicator of overall health.
Qualifications
It is important to know that a dermatologist has a full license or certification before visiting them. Some practitioners in spas and beauty clinics call themselves dermatologists but do not have the necessary accreditation.
In the U.S., a qualified dermatologist will be certified by the American Board of Dermatology, the American Osteopathic Board of Dermatology, or the Royal College of Physicians and Surgeons of Canada.
The American Academy of Dermatology (AAD) is the largest membership dermatology group in the United States, with more than 20,000 members.
To qualify for registration with the AAD, a dermatologist has to finish both college and medical school as either a medical doctor (MD) or a doctor of osteopathic medicine (DO). They will also have completed a residency involving 1 year of hands-on work.
Some dermatologists have the initials FAAD after their names. This abbreviation stands for: Fellow of the American Academy of Dermatology. It indicates that the dermatologist:
• has a license to practice medicine
• has passed exams given by either the American Board of Dermatology or the Royal College of Physicians and Surgeons of Canada
• is a member of the AAD
The AAD provide a search tool to help people with skin, hair, or nail conditions find a nearby dermatologist.
Common conditions
Being a dermatologist requires a great depth of clinical knowledge, including, for example, the various internal health problems that can cause skin symptoms.
Dermatologists can treat more than 3,000 conditions. Below are some examples of those that they see most commonly:
Acne: Among the most prevalent skin issues, acne has a range of causes that can lead to different types of pimples. Some people experience scarring, low self-esteem, and other complications.
Dermatitis and eczema: Dermatitis is inflammation of the skin, and it typically leads to swelling with an itchy rash. There are various forms, including atopic dermatitis, which is the most common type of eczema.
Fungal infections: These are common and sometimes involve the skin, nails, and hair. A group of yeasts called Candida can cause a wide range of fungal infections, including oral thrush, ringworm, athlete’s foot, and balanitis.
Hair loss: About 80 million people in the U.S. have hereditary hair loss. A range of health issues can also cause hair loss, including head lice, which affects around 6–12 million children aged 3–11 years in the U.S. annually.
Warts: These are contagious, benign skin growths that appear when a virus has infected the top layer of skin. A dermatologist can use a variety of treatments to remove persistent warts.
Nail problems: Dermatologists also treat health issues that damage the skin around and under the nails. Ingrown nails, fungal infections, and various other conditions can cause this damage.
Vitiligo: This involves the skin losing melanin, a pigment. As a result, some patches of skin are lighter in color than others.
Psoriasis: This chronic autoimmune disorder speeds up the growth of skin cells, resulting in patches of skin that may be thick, red, purple, or silvery and scaly. There are several types of psoriasis.
Rosacea: This causes redness in the face, sometimes with pus-filled bumps, visible blood vessels, and swelling of the eyelids. Symptoms can spread from the nose and cheeks to the forehead, chin, ears, chest, and back.
Shingles, or herpes zoster: This viral infection causes a rash that may be painful. It may clear in a few weeks without treatment, but medical intervention can help speed recovery and prevent complications, which can be severe.
Skin cancer: About 1 in 5 people in the U.S. develop a type of skin cancer by age 70. The most common forms are basal cell carcinoma, melanoma, and squamous cell carcinoma.
Procedures
Dermatologists use a range of medical and cosmetic procedures to manage issues affecting the skin, nails, and hair.
Medications and noninvasive therapies can treat many skin conditions, while others require more invasive approaches. These procedures can take place in an outpatient setting, such as the doctor’s office, or in a hospital.
Chemical peels
This involves applying a chemical solution that causes a layer of skin to peel off, revealing regenerated skin beneath that is typically smoother.
Dermatologists use this procedure to treat sun-damaged skin and some types of acne. It can also address cosmetic complaints, such as age spots and lines under the eyes.
Cosmetic injections
Wrinkles, scarring, and reduced facial fullness can be temporarily addressed with injections. A dermatologist can inject Botox or fillers such as collagen and fat during an office visit.
Results tend to last for a few months, and maintaining the effects requires regular injections. However, some people develop antibodies to Botox that make the injections ineffective.
Cryotherapy
Cryotherapy can be a quick treatment for many benign skin issues, such as warts.
The procedure involves freezing skin lesions — often with liquid nitrogen — to destroy the affected cells.
Dermabrasion
Dermabrasion can help reduce scar tissue, the appearance of fine wrinkles and tattoos, and potentially precancerous areas of skin.
Using a high-speed rotating brush, a dermatologist removes the top layer of skin.
Excision of lesions
Dermatologists excise skin lesions for several reasons. They may cut away these lesions:
• to prevent a disease from spreading
• for cosmetic reasons
• to prevent reoccurring infection
• to alleviate symptoms
• to diagnose an underlying issue
Depending on the size of the lesion, the person may receive a local or general anesthetic before the removal.
Hair removal or restoration
A dermatologist can use various methods to address hair loss, including transplantation.
Alternately, they can remove unwanted body hair using lasers.
Laser surgery
Dermatologists can also use laser surgery to treat a variety of skin issues or cosmetic complaints, including:
• tumors
• warts
• moles
• unwanted tattoos
• birthmarks
• scars
• wrinkles
Vein procedures
Superficial leg veins are small, dilated surface veins. People sometimes call them spider veins and may request their removal.
Sclerotherapy tends to be the spider vein treatment of choice. It involves injecting either foam or a special solution into the vein, which irritates the lining, causing the vein to shut, then become less distinct or disappear.
Tumescent liposuction
Dermatologists use tumescent liposuction to remove fat. It involves injecting large volumes of local anesthetic into fatty tissue, then sucking it from the body.
Tumescent liposuction is not a treatment for obesity — it is a cosmetic procedure for body contouring.
Dermatologists can also use lasers to selectively burst fat cells.
Skin grafts and flaps
Dermatologists can restore missing skin using skin from elsewhere on the body.
Or, they may repair skin loss by creating a flap of skin from a nearby area and using it to cover the damaged patch.
Biopsies
A dermatologist usually performs a skin biopsy to diagnose or rule out certain conditions.
They typically use one of the following three approaches:
• Shave biopsies remove small sections of the top layer of skin.
• Punch biopsies remove small, circular sections of skin, including deeper layers.
• Excision biopsies remove entire areas of skin that seem to be unhealthy.
PUVA
PUVA stands for: psoralen combined with ultraviolet A radiation. Psoralen is a drug that makes the skin more sensitive to the radiation treatment.
Dermatologists use PUVA to treat skin diseases, such as psoriasis, dermatitis, and vitiligo.
Mohs surgery
Mohs surgery is a treatment for skin cancer.
First, the dermatologist removes layers of skin to get rid of cancerous cells, then examines them under a microscope.
They then remove successive layers until there are no more cancerous cells. Performing this surgery requires specialized training.
When to see a dermatologist
If skin, hair, or nail symptoms are not responding to home treatment, it may be time to seek professional attention.
If concerns are cosmetic, a person can seek out a specialized cosmetic dermatologist.
It is important for people to discuss any upcoming dermatological treatments with their insurance providers, who often do not fund cosmetic procedures.
Be sure to obtain copies of any medical reports, consultation notes, and diagnostic test results to assure the insurer of the medical necessity of the treatment.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#987 2021-04-11 00:02:58
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
965) Pediatrician
What Is a Pediatrician?
It's one of the biggest decisions you make before your baby is born. Which pediatrician is the right one for your child? Before you start your search, take a few minutes to learn exactly what this kind of doctor does. It will help you make a better choice and know what to expect when your little one arrives.
Pediatricians are doctors who manage the health of your child, including physical, behavior, and mental health issues. They're trained to diagnose and treat childhood illnesses, from minor health problems to serious diseases.
Pediatricians have an education that gives them special skills to take care of your child's health. They graduated from medical school and completed a 3-year residency program in pediatrics.
You'll want to find one who's also "board-certified." That means they've passed rigorous exams given by the American Board of Pediatrics. To stay certified, pediatricians have to meet regular education requirements.
What Does Your Pediatrician Do?
They'll see your child many times from birth to age 2 and once a year from ages 2 to 5 for "well-child visits." After age 5, your pediatrician will likely continue to see your child every year for annual checkups. They're also the first person to call whenever your child is sick.
To take care of your child, your pediatrician will:
• Do physical exams
• Give your child vaccinations
• Make sure she meets milestones in growth, behavior, and skills
• Diagnose and treat your child's illnesses, infections, injuries, and other health problems
• Give you information about your child's health, safety, nutrition, and fitness needs
• Answer your questions about your little one's growth and development
• Refer you to specialists if they think your child needs expert care
How Does Your Pediatrician Work With Your Delivery Team?
Most hospitals ask if you have a pediatrician when you go in to deliver. Your baby's first examination may be with a hospital pediatrician or your chosen pediatrician. It depends on the hospital's policy and whether your newborn's doctor makes rounds there. If a hospital pediatrician checks your baby, they'll send your pediatrician notes about the exam.
After you leave the hospital, your pediatrician will see your baby 48 to 72 hours later, and regularly after that for checkups.
Why Do You Need a Pediatrician?
One thing to keep in mind: Family medicine doctors are also an option for your child. They look after the health of your whole family -- kids and grown-ups alike. It's a personal choice whether you use one or a pediatrician.
Some reasons to go with a pediatrician are:
• They have special training in children's health.
• They only see children in their practice, so they have a lot of experience in recognizing and treating childhood illnesses.
• If your child was born early or has a health condition that needs close monitoring, a pediatrician may offer more specialized care.
Pediatrics
Pediatrics, medical specialty dealing with the development and care of children and with the diagnosis and treatment of childhood diseases. The first important review of childhood illness, an anonymous European work called ‘The Children’s Practice’, dates from the 12th century. The specialized focus of pediatrics did not begin to emerge in Europe until the 18th century. The first specialized children’s hospitals, such as the London Foundling Hospital, established in 1745, were opened at this time. These hospitals later became major centres for training in pediatrics, which began to be taught as a separate discipline in medical schools by the middle of the 19th century.
The major focus of early pediatrics was the treatment of infectious diseases that affected children. Thomas Sydenham in Britain had led the way with the first accurate descriptions of measles, scarlet fever, and other diseases in the 17th century. Clinical studies of childhood diseases proliferated throughout the 18th and 19th centuries, culminating in one of the first modern textbooks of pediatrics, published by Frédéric Rilliet and Antoine Barthez in France in 1838–43, but there was little that could be done to cure these diseases until the end of the 19th century. As childhood diseases came under control through the combined efforts of pediatricians, immunologists, and public-health workers, the focus of pediatrics began to change, and early in the 20th century the first well-child clinics were established to monitor and study the normal growth and development of children. By the mid-20th century, the use of antibiotics and vaccines had all but eliminated most serious infectious diseases of childhood in the developed world, and infant and child mortality had fallen to the lowest levels ever. In the last half of the century, pediatrics again expanded to incorporate the study of behavioral and social as well as specifically medical aspects of child health.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#988 2021-04-12 00:02:24
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
966) Tetanus
Tetanus, also called lockjaw, acute infectious disease of humans and other animals, caused by toxins produced by the bacillus Clostridium tetani and characterized by rigidity and spasms of the voluntary muscles. The almost constant involvement of the jaw muscles accounts for the popular name of the disease.
Spores of Clostridium are distributed widely in nature, especially in soil, and may enter the body through any wound, even a superficial abrasion; puncture wounds and deep lacerations are particularly dangerous because they provide the oxygen-free environment needed for growth of the microorganism.
Both the occurrence and severity of tetanus are determined by the amount of toxin produced and the resistance of the host. The neurotoxic component, tetanospasmin, is one of the deadliest poisons known. It is believed to act on the synthesis and liberation of acetylcholine, a substance having a key role in the synaptic transmission of nerve impulses throughout the body. Once it has entered the body, the toxin rapidly spreads by way of the bloodstream or directly by a nerve to the central nervous system, where it attacks motor nerve cells and excites them to overactivity. Excessive impulses rush through the nerves to the muscles, which are thrown into severe convulsive spasm. The most common spasms occur in the muscle of the jaw, and the first sign of the illness often is stiffness of the jaw, or trismus. The muscles of the mouth are often affected, pulling the lips out and up over the teeth into a grimace, the mixture of smile and snarl that heralds the onset of the generalized convulsive stage of tetanus. Spasm of the muscles of the throat can make swallowing impossible, whereas the muscles of the larynx or of the chest wall can be thrown into such violent spasm that breathing is impossible and life is threatened. This is a common cause of death if the tetanus is untreated, but there are other effects on the heart, blood pressure, and vital brain centres that may cause death later in the disease.
The incubation period is quite variable in length—from two days to two weeks in most cases but sometimes up to three months. In general, the longer the incubation period, the milder will be the disease. Treatment of tetanus is primarily supportive. Tetanus antitoxin, which contains antibodies derived from the blood of persons who have been immunized against the disease, is given to help neutralize the toxin in the bloodstream, but it has little effect once the toxin has affected the nerve endings. Intravenous penicillin kills the organisms that remain within the wound site. Patients are usually intentionally paralyzed with drugs (such as curare) to prevent muscle spasms caused by the disease; artificial or mechanical respiration is necessary because the respiratory muscles are paralyzed. After a few weeks, when the disease is curtailed, the curare treatment is stopped and the patient begins to breathe on his own again.
Passive protection with tetanus antitoxin should be administered in all cases of injuries that may be contaminated by clostridial spores. Active immunization with tetanus toxoid (prepared by chemical modification of toxin) is a relatively slow process, requiring weeks or months to become effective, and must be renewed every few years (booster doses). A first dose should be given to every accident victim, followed by two more doses several months later. This applies also to persons who have recovered from tetanus, for an attack of the disease does not confer immunity.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#989 2021-04-13 00:13:13
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
967) Cirrhosis
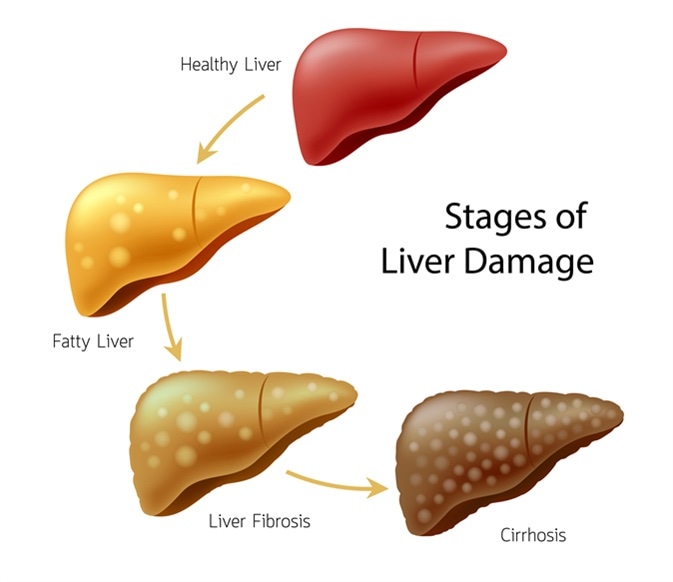
Cirrhosis, irreversible change in the normal liver tissue that results in the degeneration of functioning liver cells and their replacement with fibrous connective tissue. Cirrhosis can have a number of causes; the term is applied whenever the end result is scarring of the liver.
Laënnec, or portal, cirrhosis is primarily caused by excessive and chronic alcohol consumption. The relationship between alcohol and cirrhosis is unquestioned, but the mechanism of injury remains unknown. Besides cirrhosis, the affected person may show jaundice, gastrointestinal bleeding, and kidney failure.
In the early stage of cirrhosis, the disease can be stabilized by abstention from alcohol and by an adequate diet. In this stage, the liver first enlarges; its outer capsule becomes smooth and stretched, and its colour turns yellow because of an increase in fat. Fibrous tissue and extra bile ducts may develop. In the next stage, the quantity of fibrous tissue increases so that the liver is granular. The blood vessels thicken, and their channels may become obstructed, which reduces blood flow in the organ. Complications at this stage include coma, kidney failure, jaundice, infection, and hemorrhages. In the advanced stage of the disease, the liver shrinks and the surface usually has a roughened appearance. The normal lobular structure of the liver is lost; there is no longer fat but only poorly functioning residual liver tissue.
There are several other causes of cirrhosis besides alcohol consumption. Cirrhosis can result from viral infection, especially after infection by hepatitis B or C, glycogen storage diseases, cystic fibrosis, alpha-1-antitrypsin deficiency, and obesity can also cause cirrhosis. In hemochromatosis an increased amount of iron is absorbed by the body and deposited in the liver cells. The liver becomes granular and nodular, and the iron particles may be so dense as to impair liver cell function. In Wilson disease, a hereditary condition, there is excess copper in the liver. The liver usually turns green from bile in the tissue, and enlargement, fibrosis, fat changes, and abscesses occur when the disease is chronic.
The final complications of cirrhosis are usually the same no matter what the cause. High blood pressure in the portal vein can lead to hemorrhages in the esophagus and stomach; or the imbalance in blood chemicals from malfunctioning of the liver can affect the brain and cause hepatic coma. Hepatic coma usually starts with drowsiness and confusion and culminates in loss of consciousness. Jaundice may complicate any stage of cirrhosis. Edema—fluid retention in the tissues—and ascites, an accumulation of fluid in the peritoneal cavity that results in abdominal swelling, also are commonly seen.
Treatment of cirrhosis depends on the cause. Liver damage caused by portal cirrhosis can be halted by abstention from alcohol. Cirrhosis resulting from hepatitis infection or Wilson disease is treated with medication.
It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#990 2021-04-14 00:14:25
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
968) Scarlet fever
Scarlet fever, also called scarlatina, acute infectious disease caused by group A hemolytic streptococcal bacteria, in particular Streptococcus pyogenes. Scarlet fever can affect people of all ages, but it is most often seen in children. It is called scarlet fever because of the red skin rash that accompanies it. Before the advent of antibiotics, scarlet fever was extremely serious, often causing long periods of illness, many dangerous complications, and even death. Children with scarlet fever used to be immediately isolated and quarantined, and entire schools and neighbourhoods panicked when a case was discovered. Today, however, scarlet fever has declined in incidence and, when it does occur, in severity. Recovery is rapid and complete when antibiotics are administered promptly, and most of the potentially dangerous complications can be prevented if the full course of treatment is followed.
Scarlet fever is almost identical to streptococcal pharyngitis, commonly called strep throat, and is frequently referred to as “strep throat with a rash.” The major difference between the two illnesses is that the scarlet fever bacterium gives rise to an antigen called the erythrogenic (“redness-producing”) toxin, which is responsible for the characteristic rash.
The Course Of The Disease
Scarlet fever is rarely seen in infants and toddlers, but it begins to increase in incidence gradually after two years of age and reaches a peak incidence just before adolescence, being most common between the ages of 6 and 12. It is more common in temperate areas than in warmer tropical areas. The main sources of infection are the noses and throats of infected persons, who frequently spray droplets into the air by sneezing or coughing. Bacteria can also be transmitted indirectly by contact with contaminated objects or the unwashed hands of an infected person.
The incubation period of the scarlet fever bacterium ranges between one and seven days. The illness usually begins with a sudden onset of fever, vomiting, and severe sore throat. Along with these symptoms the child usually develops a headache, chills, and weakness. Between 12 and 24 hours after the onset of fever, the typical scarlet rash appears. Occasionally the child complains of severe abdominal pain.
In a typical case the temperature rises to 39.5 °C (103 °F) or higher. The throat is red and sore, and the tonsils are enlarged, reddened, and covered with patches of exudate. The glands under the angles of the jaw become swollen and tender. The tongue changes its appearance as the disease progresses. At the start the tip and edges are reddened, and the rest of the tongue has a whitish appearance. By the third or fourth day the white coat has peeled off, and the tongue then develops a red “strawberry” appearance.
The scarlet fever rash, which appears shortly after the fever, has been described as a “sunburn with goose pimples.” The skin is covered with tiny red spots that blanch on pressure and has a rough, sandpaper-like texture. This scarlet rash usually covers the entire body except for the area around the mouth, which remains pale. One of the most characteristic features of the rash is desquamation, or peeling, which occurs at the end of the first week. Desquamating skin comes off as fine flakes like bran. The hands and feet are usually the last to desquamate—not until the second or third week of the illness.
Diagnosis And Treatment
Most cases of scarlet fever can be diagnosed by the typical signs and symptoms alone. The most useful means of confirming a diagnosis is throat culture. Group A hemolytic streptococci can be isolated from the throat or nose by using a cotton swab, and the results of the culture can be determined after only 24 hours of incubation. Blood samples can also be drawn and checked for elevated white blood cell levels or for antibodies to various of the toxins given off by the streptococci, but these tests are rarely needed for diagnosis.
A number of antibiotics are effective in the treatment of group A streptococcal infections, but penicillin remains the drug of choice. The drug can be given by injection or by mouth. Treatment consistently results in rapid reduction of fever and improvement in well-being. The aim is to maintain an adequate blood level of penicillin against the bacteria for at least 10 days of treatment. The danger is that often, with the child feeling better after only two or three days, treatment is stopped too soon. For this reason doctors occasionally treat patients by injection of a single long-acting penicillin preparation. For children who are allergic to penicillin, there are a number of other equally effective antibiotics—for example, erythromycin.
Complications
Early complications of scarlet fever generally occur during the first week of illness. The infection may spread, causing inflammation of the middle ear (otitis media), the paranasal sinuses (sinusitis), or the lymph nodes of the neck. A rare early complication is bronchial pneumonia. Even rarer are osteomyelitis (infection of the bone), mastoiditis (infection of the bony areas behind the ears), and septicemia (blood poisoning). If the child is adequately treated, such complications rarely develop.
Of great importance are two serious late complications, rheumatic fever (inflammation of the heart and joints) and glomerulonephritis (inflammation of the urine-producing structures of the kidney). These late complications are probably caused by an autoimmune reaction brought on by the streptococci or some of their by-products. Onset varies from one to two weeks for glomerulonephritis and from two to four weeks for rheumatic fever. They may follow a mild streptococcal infection just as often as a severe one.
Rheumatic fever is relatively uncommon but serious. The incidence is said to be about 3 percent after a case of streptococcal infection that is inadequately treated and less than 1 percent after full treatment. Rheumatic fever is rarely seen in children under three years of age. Since rheumatic fever often causes damage to the heart, it is extremely important that any child with a streptococcal infection be correctly diagnosed and adequately treated.
Glomerulonephritis (also called Bright disease) is a more-common late complication. A child who develops acute glomerulonephritis has fever, blood in the urine, puffiness in the face, and, occasionally, high blood pressure. However, in most cases the prognosis for full recovery is excellent.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#991 2021-04-15 00:16:23
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
969) Adaptation
Adaptation, in biology, the process by which a species becomes fitted to its environment; it is the result of natural selection’s acting upon heritable variation over several generations. Organisms are adapted to their environments in a great variety of ways: in their structure, physiology, and genetics, in their locomotion or dispersal, in their means of defense and attack, in their reproduction and development, and in other respects.
The word adaptation does not stem from its current usage in evolutionary biology but rather dates back to the early 17th century, when it indicated a relation between design and function or how something fits into something else. In biology this general idea has been coopted so that adaptation has three meanings. First, in a physiological sense, an animal or plant can adapt by adjusting to its immediate environment—for instance, by changing its temperature or metabolism with an increase in altitude. Second, and more commonly, the word adaptation refers either to the process of becoming adapted or to the features of organisms that promote reproductive success relative to other possible features. Here the process of adaptation is driven by genetic variations among individuals that become adapted to—that is, have greater success in—a specific environmental context. A classic example is shown by the melanistic (dark) phenotype of the peppered moth (Biston betularia), which increased in numbers in Britain following the Industrial Revolution as dark-coloured moths appeared cryptic against soot-darkened trees and escaped predation by birds. The process of adaptation occurs through an eventual change in the gene frequency relative to advantages conferred by a particular characteristic, as with the coloration of wings in the moths.
The third and more popular view of adaptation is in regard to the form of a feature that has evolved by natural selection for a specific function. Examples include the long necks of giraffes for feeding in the tops of trees, the streamlined bodies of aquatic fish and mammals, the light bones of flying birds and mammals, and the long daggerlike canine teeth of carnivores.
All biologists agree that organismal traits commonly reflect adaptations. However, much disagreement has arisen over the role of history and constraint in the appearance of traits as well as the best methodology for showing that a trait is truly an adaptation. A trait may be a function of history rather than adaptation. The so-called panda’s thumb, or radial sesamoid bone, is a wrist bone that now functions as an opposable thumb, allowing giant pandas to grasp and manipulate bamboo stems with dexterity. The ancestors of giant pandas and all closely related species, such as black bears, raccoons, and red pandas, also have sesamoid bones, though the latter species do not feed on bamboo or use the bone for feeding behaviour. Therefore, this bone is not an adaptation for bamboo feeding.
The English naturalist Charles Darwin, in ‘On the Origin of Species by Means of Natural Selection’ (1859), recognized the problem of determining whether a feature evolved for the function it currently serves:
“The sutures of the skulls of young mammals have been advanced as a beautiful adaptation for aiding parturition [birth], and no doubt they facilitate, or may be indispensable for this act; but as sutures occur in the skulls of young birds and reptiles, which only have to escape from a broken egg, we may infer that this structure has arisen from the laws of growth, and has been taken advantage of in the parturition of the higher animals.”
Thus, before explaining that a trait is an adaptation, it is necessary to identify whether it is also shown in ancestors and therefore may have evolved historically for different functions from those that it now serves.
Another problem in designating a trait as an adaptation is that the trait may be a necessary consequence, or constraint, of physics or chemistry. One of the most common forms of constraint involves the function of anatomical traits that differ in size. For example, canine teeth are larger in carnivores than in herbivores. This difference in size is often explained as an adaptation for predation. However, the size of canine teeth is also related to overall body size (such scaling is known as allometry), as shown by large carnivores such as leopards that have bigger canines than do small carnivores such as weasels. Thus, differences in many animal and plant characteristics, such as the sizes of young, duration of developmental periods (e.g., gestation, longevity), or patterns and sizes of tree leaves, are related to physical size constraints.
Adaptive explanations in biology are difficult to test because they include many traits and require different methodologies. Experimental approaches are important for showing that any small variability, as in many physiological or behavioral differences, is an adaptation. The most rigorous methods are those that combine experimental approaches with information from natural settings—for example, in showing that the beaks of different species of Galapagos finch are shaped differently because they are adapted to feed on seeds of different sizes.
The comparative method, using comparisons across species that have evolved independently, is an effective means for studying historical and physical constraints. This approach involves using statistical methods to account for differences in size (allometry) and evolutionary trees (phylogenies) for tracing trait evolution among lineages.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#992 2021-04-16 00:22:05
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
970) Pyrheliometer
A pyrheliometer is an instrument for measurement of direct beam solar irradiance. Sunlight enters the instrument through a window and is directed onto a thermopile which converts heat to an electrical signal that can be recorded. The signal voltage is converted via a formula to measure watts per square metre.
Standards
Pyrheliometer measurement specifications are subject to International Organization for Standardization (ISO) and World Meteorological Organization (WMO) standards. Comparisons between pyrheliometers for intercalibration are carried out regularly to measure the amount of solar energy received. The aim of the International Pyrheliometer Comparisons, which take place every 5 years at the World Radiation Centre in Davos, is to ensure the world-wide transfer of the World Radiometric Reference. During this event, all participants bring their instruments, solar-tracking and data acquisition systems to Davos to conduct simultaneous solar radiation measurements with the World Standard Group.
Applications
Typical pyrheliometer measurement applications include scientific meteorological and climate observations, material testing research, and assessment of the efficiency of solar collectors and photovoltaic devices.
Usage
Pyrheliometers are typically mounted on a solar tracker. As the pyrheliometer only 'sees' the solar disk, it needs to be placed on a device that follows the path of the sun.
A pyrheliometer is a device used to quantify the direct sunbeam of solar insolation. Sunrays enter the windowpanes and are oriented onto an instrument called a thermopile.
A thermopile consists of thermocouples, which are connected in series. These are also, commonly referred to as Parallel. A thermopile transmutes thermal energy into electric signals. A pyrheliometer is a measuring instrument, which uses a formula to convert signal voltage to calculate watts per squared meter.
Pyrheliometer used with solar tracking systems.
A pyrheliometer is used in combination with a Solar Tracking system. This helps in keeping the instrument aimed at the sun.
The International Organization for Standardization and the World Meteorological Organization stipulates the standards for Pyrheliometer measurements. To measure the quantity of solar energy coming in directly from the Sun, regular comparisons are made between different Pyrheliometers. Also these standards are applied to intercalibrate these instruments.
The main objective of International Pyrheliometer Comparisons, which is conducted after every five years, at the World Radiation Center, situated in Davos is to assure the transfer of World Radiometric Reference across the world. All participants bring their solar tracking devices, instruments and all other acquisition systems while the event is being conducted at Davos. With these instruments, solar radiations are simultaneously measured with the World Standard Group.
Pyrheliometer usages
A typical pyrheliometer is used for meteorological, scientific and climatic observations. It also evaluates and assesses the effectiveness of Photovoltaic instruments and solar collectors.
There are two types of Pyrheliometers:
SHP1: it is a pyrheliometer device well equipped with an interface having both digitized RS 485 Modbus and an intensified analogue output. This pyrheliometer offers a smart interface and is an advancement of the CPH 1 version. Moreover, the SHP1 also has a response period below 2 seconds. The individually measure temperature correction varies from negative 40°C to positive 70°C.
CHP 1: This type of pyrheilometer completely complies with the latest standards set by International Standardization Organization (ISO) and World Meteorological Organization (WMO) regarding the criteria for First Class Normal Incidence Pyrheliometer. Each pyrheliometer is checked for manufacturing and supply standards with a traceable checking certificate issued by the World Radiometric Reference (WRD).
Concluding
Pyrheliometer is generally used to analyze the variations in solar radiation productivity. Another function of the pyrheliometer is the solar panel design and placement.
Different amounts of solar irradiance reaches diverse parts of the Earth, so these pyrheilometers come in handy to create average radiation level maps. With the creation of these maps, the appropriate placement of solar panels can be identified.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#993 2021-04-17 00:22:00
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
971) Pressure cooker
Pressure cooker, hermetically sealed pot which produces steam heat to cook food quickly. The pressure cooker first appeared in 1679 as Papin’s Digester, named for its inventor, the French-born physicist Denis Papin. The cooker heats water to produce very hot steam which forces the temperature inside the pot as high as 266° F (130° C), significantly higher than the maximum heat possible in an ordinary saucepan. The higher temperature of a pressure cooker penetrates food quickly, reducing cooking time without diminishing vitamin and mineral content.
Pressure cookers are especially useful at high altitudes, where they alleviate the problem of low temperature boiling caused by reduced atmospheric pressure.
Modern innovations in pressure cooker design include safety locks, pressure regulators, portable cookers, and low-pressure fryers.
Boiling
Boiling, the cooking of food by immersion in water that has been heated to near its boiling point (212 °F [100 °C] at sea level; at higher altitudes water boils at lower temperatures, the decrease in boiling temperature being approximately one degree Celsius for each 1,000 feet [300 metres]). Water-soluble substances, such as sugar and salt, raise the boiling point of the water).
Boiling is used primarily to cook meats and vegetables. The extent of cooking varies according to individual taste and regional or traditional dictum; in the cookery of the U.S. South, for example, the boiling of vegetables is usually protracted, with a soft consistency and a blend of flavours in combined ingredients considered desirable. In the nouvelle cuisine of France, on the other hand, Chinese influence dictates minimal boiling or steaming to preserve fresh colour, texture, and flavour.
A number of specific terms apply to methods of cooking with hot water. Scalding is accomplished in water heated to around 185 °F (85 °C), usually in a double boiler, which conducts the heat of the water, contained in a bigger pan, to a smaller pan containing the food, thus avoiding contact between food and water. This technique is commonly used to prepare milk for breads and custards. At just above the scalding temperature, water begins to circulate visibly and to shiver; at this point, foods, notably eggs and fish, may be poached. At the simmering point, variously specified but generally approaching the boiling temperature, the surface of the water breaks into small bubbles; simmering, in a covered or open pan, is commonly used to prepare soups, stews, and pot roasts. In blanching, boiling water is poured over vegetables, fruits, or nutmeats in order to loosen the outer skin. Parblanching or parboiling consists in immersing the food in cold water and then bringing it slowly to a simmer or boil.
Steaming comprises two related techniques, both used primarily for the cooking of vegetables. In the first, the food is placed on a rack above a shallow portion of water, heated to the boil, in a covered pan; this method is valued for its preservation of colour, texture, flavour, and nutrients. The second technique, called pressure cooking, requires a tightly sealed, often latched, vessel, in which characteristically tough or long-cooking foods may be subjected to steam cooking under high pressure. The classic New England boiled dinner, consisting of corned beef cooked with cabbage, carrots, potatoes, and onions, is traditionally boiled in the conventional manner but may be adapted readily to pressure cooking.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#994 2021-04-18 00:02:27
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
972) Psychiatry
Psychiatry, the science and practice of diagnosing, treating, and preventing mental disorders.
The term psychiatry is derived from the Greek words psyche, meaning “mind” or “soul,” and iatreia, meaning “healing.” Until the 18th century, mental illness was most often seen as demonic possession, but it gradually came to be considered as a sickness requiring treatment. Many judge that modern psychiatry was born with the efforts of French physician Philippe Pinel in the late 1700s. His contemporary in the United States, statesman and physician Benjamin Rush, introduced a comparable approach. Perhaps the most significant contributions to the field occurred in the late 19th century, when German psychiatrist Emil Kraepelin emphasized a systematic approach to psychiatric diagnosis and classification and Austrian psychoanalyst Sigmund Freud, who was familiar with neuropathology, developed psychoanalysis as a treatment and research approach.
In countries such as the United States and the United Kingdom, psychiatrists have both a bachelor’s degree and a medical degree and at least four years of specialty training in psychiatry. In the United States and Canada, specialty training occurs during a period of residency, which typically begins with work in a hospital setting in which the resident learns to provide supervised care to acutely ill individuals. Following this period of hospital training, which lasts at least one year, residents are required to complete an additional three or more years of training that includes designated clinical and didactic experiences. These experiences must take place in structured educational programs that expose the resident to the biological, psychological, and sociocultural determinants of the major psychiatric disorders. Graduates of residency programs in the United States and Canada or of equivalent programs in other countries are designated as having achieved the knowledge, skills, and attitudes of the profession. These individuals have the ability to address the complicated ethical questions that often arise in the care of patients whose capacity for participation in their own treatment may be compromised. In many countries, before psychiatrists can begin practicing, they must take and pass both written and oral examinations. In the United States, successful completion of these exams enables psychiatrists to become board certified, meaning they have met the national benchmark criteria of competency required for the practice of psychiatry.
Certified psychiatrists should be able to employ treatments, such as drug therapy, electroconvulsive therapy, and biofeedback, to address biological dimensions of mental and emotional disorders. In addition, they should be prepared to apply different forms of psychotherapy, such as cognitive behavioral or interpersonal psychotherapies, to the psychological elements of mental and emotional dysfunction. Certified psychiatrists must be able to combine different treatments based on their understanding of the complexities of mind-brain interactions; this often involves an understanding of environmental factors and of how these factors apply to individuals with severe and persistent mental illness. Most mental and emotional disorders require a pluralistic treatment approach because they affect so many facets of the human experience. As a result, psychiatrists frequently work as part of a multidisciplinary treatment team with psychologists, social work professionals, occupational therapists, and psychiatric nurses.
In addition to overall competency to deal with psychiatric disorders, some psychiatrists pursue subspecialty training and associated certification. Examples of subspecialties include addiction psychiatry, forensic psychiatry, geriatric psychiatry, and psychosomatic psychiatry. Subspecialty education typically involves an additional one to two years of training. Other forms of subspecialty education, which are not recognized by board certification in the United States, include fellowships in emergency psychiatry and in neuropsychiatry, which focuses on the treatment of psychiatric symptoms in individuals with neurological disorders, such as traumatic brain injury and stroke.
There has been rapid growth in the science of psychiatry because of the development of technology that allows measurement and observation of brain function. Neuroimaging techniques, such as magnetic resonance imaging (MRI), positron emission tomography (PET), and single photon emission computed tomography (SPECT), have begun to answer basic questions about both psychopathologic disorders and normal development and function. These technologies can be used to integrate the different dimensions of the biopsychosocial model—biology, psychology, and sociology—that have been characterized independently.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#995 2021-04-19 00:03:05
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
973) Extrasensory perception - 1
Extrasensory perception or ESP, also called sixth sense, includes claimed reception of information not gained through the recognized physical senses, but sensed with the mind. The term was adopted by Duke University psychologist J. B. Rhine to denote psychic abilities such as intuition, telepathy, psychometry, clairvoyance, and their trans-temporal operation as precognition or retrocognition.
Second sight is a form of extrasensory perception, the power to perceive things that are not present to the 5 senses, whereby a person perceives information, in the form of a vision, about future events before they happen (precognition), or about things or events at remote locations (remote viewing). There is no scientific evidence that second sight exists. Reports of second sight are known only from anecdotal evidence given after the fact.
History
In the 1930s, at Duke University in North Carolina, J. B. Rhine and his wife Louisa E. Rhine conducted investigation into extrasensory perception. While Louisa Rhine concentrated on collecting accounts of spontaneous cases, J. B. Rhine worked largely in the laboratory, carefully defining terms such as ESP and psi and designing experiments to test them. A simple set of cards was developed, originally called Zener cards – now called ESP cards. They bear the symbols circle, square, wavy lines, cross, and star. There are five of each type of card in a pack of 25.
In a telepathy experiment, the "sender" looks at a series of cards while the "receiver" guesses the symbols. To try to observe clairvoyance, the pack of cards is hidden from everyone while the receiver guesses. To try to observe precognition, the order of the cards is determined after the guesses are made. Later he used dice to test for psychokinesis.
The parapsychology experiments at Duke evoked criticism from academics and others who challenged the concepts and evidence of ESP. A number of psychological departments attempted, unsuccessfully, to repeat Rhine's experiments. W. S. Cox (1936) from Princeton University with 132 subjects produced 25,064 trials in a playing card ESP experiment. Cox concluded "There is no evidence of extrasensory perception either in the 'average man' or of the group investigated or in any particular individual of that group. The discrepancy between these results and those obtained by Rhine is due either to uncontrollable factors in experimental procedure or to the difference in the subjects." Four other psychological departments failed to replicate Rhine's results.
In 1938, the psychologist Joseph Jastrow wrote that much of the evidence for extrasensory perception collected by Rhine and other parapsychologists was anecdotal, biased, dubious and the result of "faulty observation and familiar human frailties". Rhine's experiments were discredited due to the discovery that sensory leakage or cheating could account for all his results such as the subject being able to read the symbols from the back of the cards and being able to see and hear the experimenter to note subtle clues.
In the 1960s parapsychologists became increasingly interested in the cognitive components of ESP, the subjective experience involved in making ESP responses, and the role of ESP in psychological life. This called for experimental procedures that were not limited to Rhine's favored forced-choice methodology. Such procedures have included dream telepathy experiments, and the ganzfeld experiments (a mild sensory deprivation procedure).
Second sight may have originally been so called because normal vision was regarded as coming first, while supernormal vision is a secondary thing, confined to certain individuals. ‘An dà shealladh’ or "the two sights", meaning "the sight of the seer", is the way Gaels refer to "second sight", the involuntary ability of seeing the future or distant events. There are many Gaelic words for the various aspects of second sight, but ‘an dà shealladh’ is the one mostly recognized by non-Gaelic speakers, even though, strictly speaking, it does not really mean second sight, but rather "two sights".
Skepticism
Parapsychology is the study of paranormal psychic phenomena, including ESP. Parapsychology has been criticized for continuing investigation despite being unable to provide convincing evidence for the existence of any psychic phenomena after more than a century of research. The scientific community rejects ESP due to the absence of an evidence base, the lack of a theory which would explain ESP and the lack of positive experimental results; it considers ESP to be pseudoscience.
The scientific consensus does not view extrasensory perception as a scientific phenomenon. Skeptics have pointed out that there is no viable theory to explain the mechanism behind ESP, and that there are historical cases in which flaws have been discovered in the experimental design of parapsychological studies.
There are many criticisms pertaining to experiments involving extrasensory perception, particularly surrounding methodological flaws. These flaws are not unique to a single experimental design, and are effective in discrediting much of the positive research surrounding ESP. Many of the flaws seen in the Zener cards experiment are present in the Ganzfeld experiment as well. First is the stacking effect, an error that occurs in ESP research. Trial-by-trial feedback given in studies using a “closed” ESP target sequence (e.g., a deck of cards) violates the condition of independence used for most standard statistical tests. Multiple responses for a single target cannot be evaluated using statistical tests that assume independence of responses. This increases likelihood of card counting and in turn, increases the chances for the subject to guess correctly without using ESP. Another methodological flaw involves cues through sensory leakage. For example, when the subject receives a visual cue. This could be the reflection of a Zener card in the holder's glasses. In this case, the subject is able to guess the card correctly because they can see it in the reflection, not because of ESP. Finally, poor randomization of target stimuli could be happening. Poor shuffling methods can make the orders of the cards easier to predict, or the cards could’ve been marked and manipulated, again, making it easier to predict which cards come next. The results of a meta-analysis found that when these errors were corrected and accounted for, there was still no significant effect of ESP. Many of the studies only appeared to have significant occurrence of ESP, when in fact, this result was due to the many methodological errors in the research.
Dermo-optical perception
In the early 20th century, Joaquin María Argamasilla, known as the "Spaniard with X-ray Eyes", claimed to be able to read handwriting or numbers on dice through closed metal boxes. Argamasilla managed to fool Gustav Geley and Charles Richet into believing he had genuine psychic powers. In 1924, he was exposed by Harry Houdini as a fraud. Argamasilla peeked through his simple blindfold and lifted up the edge of the box so he could look inside it without others noticing.
Science writer Martin Gardner has written that the ignorance of blindfold deception methods has been widespread in investigations into objects at remote locations from persons who claim to possess second sight. Gardner documented various conjuring techniques psychics such as Rosa Kuleshova, Lina Anderson and Nina Kulagina have used to peek from their blindfolds to deceive investigators into believing they used second sight.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#996 2021-04-20 00:23:30
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
974) Extrasensory perception – 2
Categories
Extrasensory perception (ESP), perception that occurs independently of the known sensory processes. Usually included in this category of phenomena are telepathy, or thought transference between persons; clairvoyance, or supernormal awareness of objects or events not necessarily known to others; and precognition, or knowledge of the future. Scientific investigation of these and similar phenomena dates from the late 19th century, with most supporting evidence coming from experiments involving card guessing. Subjects attempt to guess correctly the symbols of cards hidden from their view under controlled conditions; a better-than-chance percentage of correct calls on a statistically significant number of trials is considered to be evidence of ESP. Although many scientists continue to doubt the existence of ESP, people who claim this ability are sometimes used by investigative teams searching for missing persons or things.
Telepathy
Telepathy, direct transference of thought from one person (sender or agent) to another (receiver or percipient) without using the usual sensory channels of communication, hence a form of extrasensory perception (ESP). While the existence of telepathy has not yet been proved, some parapsychological research studies have produced favourable results using such techniques as card guessing with a special deck of five sets of five cards. The agent may simply think of a random order of the five card symbols while the percipient tries to think of the order on which the agent is concentrating. In a general ESP test the sender concentrates on the face of one card at a time while the receiver tries to think of the symbol. Both subjects are, of course, separated by a screen or some greater obstacle or distance. Scores significantly above chance are extremely rare, particularly as testing methods have become more rigorous.
Clairvoyance
Clairvoyance, (French: “clear seeing”) knowledge of information not necessarily known to any other person, not obtained by ordinary channels of perceiving or reasoning—thus a form of extrasensory perception (ESP). Spiritualists also use the term to mean seeing or hearing (clairaudience) the spirits of the dead that are said to surround the living. Research in parapsychology—such as testing a subject’s ability to predict the order of cards in a shuffled deck—has yet to provide conclusive support for the existence of clairvoyance.
Precognition
Precognition, supernormal knowledge of future events, with emphasis not upon mentally causing events to occur but upon predicting those the occurrence of which the subject claims has already been determined. Like telepathy and clairvoyance, precognition is said to operate without recourse to the normal senses and thus to be a form of extrasensory perception (ESP).
There is a long tradition of anecdotal evidence for foreseeing the future in dreams and by various devices such as observing the flight of birds or examining the entrails of sacrificial animals. Precognition has been tested with subjects required to predict the future order of cards in a deck about to be shuffled or to foretell results of dice throws, but the statistical support for it has generally been less convincing than that from experiments in telepathy and clairvoyance.
Psychokinesis
Psychokinesis, also called telekinesis, in parapsychology, the action of mind on matter, in which objects are supposedly caused to move or change as a result of mental concentration upon them. The physical nature of psychokinetic effects contrasts with the cognitive quality of extrasensory perception (ESP), the other major grouping of parapsychological phenomena. Claimed effects of psychokinesis include levitation and metal bending; such displays are common, though fraudulent, in theatrical magic.
Despite experimental investigation, scientific evidence supporting the existence of psychokinesis is lacking. In an example of a psychokinetic test, the subject attempts by thinking or willing to influence thrown dice, causing a certain die face to turn up or causing the die to land in a certain area. Other experiments have focused on the ability of subjects to influence outcomes of random number generators. Some researchers have interpreted the results of such experiments as revealing the existence of very small effects in which consciousness influences outcomes in such random physical systems. Other studies, however, indicate that such conclusions are the result of various forms of bias, including publication bias and confirmation bias. Hence, experimental results, as with other parapsychological phenomena, have been inconclusive.
Parapsychology
Parapsychology, Discipline concerned with investigating events that cannot be accounted for by natural law and knowledge that cannot have been obtained through the usual sensory abilities. Parapsychology studies the cognitive phenomena often called extrasensory perception, in which a person acquires knowledge of other people’s thoughts or of future events through channels apparently beyond the five senses. It also examines physical phenomena such as the levitation of objects and the bending of metal through psychokinesis. Though belief in such phenomena may be traced to earliest times, parapsychology as a subject of serious research originated in the late 19th century, partly in reaction to the growth of the spiritualist movement. The Society of Psychical Research was established in London in 1882, and similar societies were later founded in the U.S. and in many European countries. In the 20th century research into parapsychology was also conducted at some universities, notably at Duke University under J. B. Rhine.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#997 2021-04-21 00:09:03
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
975) Amplifier
Amplifier, in electronics, device that responds to a small input signal (voltage, current, or power) and delivers a larger output signal that contains the essential waveform features of the input signal. Amplifiers of various types are widely used in such electronic equipment as radio and television receivers, high-fidelity audio equipment, and computers. Amplifying action can be provided by electromechanical devices (e.g., transformers and generators) and vacuum tubes, but most electronic systems now employ solid-state microcircuits as amplifiers. Such an integrated circuit consists of many thousands of transistors and related devices on a single tiny silicon chip.
A single amplifier is usually insufficient to raise the output to the desired level. In such cases the output of the first amplifier is fed into a second, whose output is fed to a third, and so on, until the output level is satisfactory. The result is cascade, or multistage amplification. Long-distance telephone, radio, television, electronic control and measuring instruments, radar, and countless other devices all depend on this basic process of amplification. The overall amplification of a multistage amplifier is the product of the gains of the individual stages.
There are various schemes for the coupling of cascading electronic amplifiers, depending upon the nature of the signal involved in the amplification process. Solid-state microcircuits have generally proved more advantageous than vacuum-tube circuits for the direct coupling of successive amplifier stages. Transformers can be used for coupling, but they are bulky and expensive.
An electronic amplifier can be designed to produce a magnified output signal identical in every respect to the input signal. This is linear operation. If the output is altered in shape after passing through the amplifier, amplitude distortion exists. If the amplifier does not amplify equally at all frequencies, the result is called frequency distortion, or discrimination (as in emphasizing bass or treble sounds in music recordings).
When the power required from the output of the amplifier is so large as to preclude the use of electronic devices, dynamoelectric and magnetic amplifiers find wide application.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#998 2021-04-22 00:18:37
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
976) Atomic Mass Unit Definition (AMU)
In chemistry, an atomic mass unit or AMU is a physical constant equal to one-twelfth of the mass of an unbound atom of carbon-12. It is a unit of mass used to express atomic masses and molecular masses. When the mass is expressed in AMU, it roughly reflects the sum of the number of protons and neutrons in the atomic nucleus (electrons have so much less mass that they are assumed to have a negligible effect). The symbol for the unit is u (unified atomic mass unit) or Da (Dalton), although AMU may still be used.
1 u = 1 Da = 1 amu (in modern usage) = 1 g/mol
Also Known As: unified atomic mass unit (u), Dalton (Da), universal mass unit, either amu or AMU is an acceptable acronym for atomic mass unit
The "unified atomic mass unit" is a physical constant that is accepted for use in the SI measurement system. It replaces the "atomic mass unit" (without the unified part) and is the mass of one nucleon (either a proton or a neutron) of a neutral carbon-12 atom in its ground state. Technically, the amu is the unit that was based on oxygen-16 until 1961, when it was redefined based on carbon-12. Today, people use the phrase "atomic mass unit," but what they mean is "unified atomic mass unit."
One unified atomic mass unit is equal to:
• 1.66 yoctograms
• 1.66053904020 x {10}^{-27} kg
• 1.66053904020 x {10}^{-24} g
• 931.49409511 MeV/c2
• 1822.8839 me
History of the Atomic Mass Unit
John Dalton first suggested a means of expressing relative atomic mass in 1803. He proposed the use of hydrogen-1 (protium). Wilhelm Ostwald suggested that relative atomic mass would be better if expressed in terms of 1/16th the mass of oxygen. When the existence of isotopes was discovered in 1912 and isotopic oxygen in 1929, the definition based on oxygen became confusing. Some scientists used an AMU based on the natural abundance of oxygen, while others used an AMU based on the oxygen-16 isotope. So, in 1961 the decision was made to use carbon-12 as the basis for the unit (to avoid any confusion with an oxygen-defined unit). The new unit was given the symbol u to replace amu, plus some scientists called the new unit a Dalton. However, u and Da were not universally adopted. Many scientists kept using the amu, just recognizing it was now based on carbon rather than oxygen. At present, values expressed in u, AMU, amu, and Da all describe the exact same measure.
Examples of Values Expressed in Atomic Mass Units
• A hydrogen-1 atom has a mass of 1.007 u (or Da or amu).
• A carbon-12 atom is defined as having a mass of 12 u.
• The largest known protein, titin, has a mass of 3 x 106 Da.
• AMU is used to differentiate between isotopes. An atom of U-235, for example, has a lower AMU than one of U-238, since they differ by the number of neutrons in the atom.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#999 2021-04-23 00:06:49
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
977) Acrophobia
Acrophobia is an extreme or irrational fear or phobia of heights, especially when one is not particularly high up. It belongs to a category of specific phobias, called space and motion discomfort, that share both similar causes and options for treatment.
Most people experience a degree of natural fear when exposed to heights, known as the fear of falling. On the other hand, those who have little fear of such exposure are said to have a head for heights. A head for heights is advantageous for those hiking or climbing in mountainous terrain and also in certain jobs such as steeplejacks or wind turbine mechanics.
People with acrophobia can experience a panic attack in high places and become too agitated to get themselves down safely. Approximately 2–5% of the general population has acrophobia, with twice as many women affected as men. The term is from the Greek: ákron, meaning "peak, summit, edge" and phóbos, "fear".
Confusion with vertigo
"Vertigo" is often used (incorrectly) to describe a fear of heights, but it is more accurately a spinning sensation that occurs when one is not actually spinning. It can be triggered by looking down from a high place, by looking straight up at a high place or tall object, or even by watching something (i.e. a car or a bird) go past at high speed, but this alone does not describe vertigo. True vertigo can be triggered by almost any type of movement (e.g. standing up, sitting down, walking) or change in visual perspective (e.g. squatting down, walking up or downstairs, looking out of the window of a moving car or train). Vertigo is called height vertigo when the sensation of vertigo is triggered by heights.
Height vertigo is caused by a conflict between vision, vestibular and somatosensory senses. This occurs when vestibular and somatosensory systems sense a body movement that is not detected by the eyes. More research indicate that this conflict lead to both motion sickness and anxiety.
Causes
Traditionally, acrophobia has been attributed, like other phobias, to conditioning or a traumatic experience. Recent studies have cast doubt on this explanation. Individuals with acrophobia are found to be lacking in traumatic experiences. Nevertheless, this may due to the failure to recall the experiences, as memory fades as time passes. To address the problems of self report and memory, a large cohort study with 1000 participants was conducted from birth; the results showed that participants with less fear of heights had more injuries because of falling. More studies have suggested a possible explanation for acrophobia is that it emerges through accumulation of non-traumatic experiences of falling that are not memorable but can influence behaviours in the future. Also, fear of heights may be acquired when infants learn to crawl. If they fell, they would learn the concepts about surfaces, posture, balance, and movement. Coginitive factors may also contribute to the development of acrophobia. People tend to wrongly interpret visuo-vestibular discrepancies as dizziness and nausea and associate them with a forthcoming fall. A traumatic conditional event of falling may not be necessary at this point.
A fear of falling, along with a fear of loud noises, is one of the most commonly suggested inborn or "non-associative" fears. The newer non-association theory is that a fear of heights is an evolved adaptation to a world where falls posed a significant danger. If this fear is inherited, it is possible that people can get rid of it by frequent exposure of heights in habituation. In other words, acrophobia could be attributed to the lack of exposure in early times. The degree of fear varies and the term phobia is reserved for those at the extreme end of the spectrum.
Researchers have argued that a fear of heights is an instinct found in many mammals, including domestic animals and humans. Experiments using visual cliffs have shown human infants and toddlers, as well as other animals of various ages, to be reluctant in venturing onto a glass floor with a view of a few meters of apparent fall-space below it. Although human infants initially experienced fear when crawling on the visual cliff, most of them overcame the fear through practice, exposure and mastery and retained a level of healthy cautiousness. While an innate cautiousness around heights is helpful for survival, an extreme fear can interfere with the activities of everyday life, such as standing on a ladder or chair, or even walking up a flight of stairs. Still, it is uncertain if acrophobia is related to the failure to reach a certain developmental stage. Besides associative accounts, a diathetic-stress model is also very appealing for considering both vicarious learning and hereditary factors such as personality traits (i.e., neuroticism).
Another possible contributing factor is a dysfunction in maintaining balance. In this case the anxiety is both well founded and secondary. The human balance system integrates proprioceptive, vestibular and nearby visual cues to reckon position and motion. As height increases, visual cues recede and balance becomes poorer even in normal people. However, most people respond by shifting to more reliance on the proprioceptive and vestibular branches of the equilibrium system.
Some people are known to be more dependent on visual signals than others. People who rely more on visual cues to control body movements are less physically stable. An acrophobic, however, continues to over-rely on visual signals whether because of inadequate vestibular function or incorrect strategy. Locomotion at a high elevation requires more than normal visual processing. The visual cortex becomes overloaded, resulting in confusion. Some proponents of the alternative view of acrophobia warn that it may be ill-advised to encourage acrophobics to expose themselves to height without first resolving the vestibular issues. Research is underway at several clinics. Recent studies found that participants experienced increased anxiety not only during elevation in height, but also when they were required to move sideways in a fixed height.
A recombinant model of the development of acrophobia is very possible, in which learning factors, cognitive factors (e.g. interpretations), perceptual factors(e.g. visual dependence), and biological factors (e.g. heredity) interact to provoke fear or habituation.
Assessment
ICD-10 and DSM-V are used to diagnose acrophobia. Acrophobia Questionnaire (AQ) is a self report that contains 40 items, assessing anxiety level on a 0-6 point scale and degree of avoidance on a 0-2 point scale. The Attitude Towards Heights Questionnaires (ATHQ) and Behavioural Avoidance Tests (BAT) are also used.
However, acrophobic individuals tend to have biases in self report. They often overestimate the danger and question their abilities of addressing height relevant issues. A Height Interpretation Questionnaire (HIQ) is a self-report to measure these height relevant judgements and interpretations. The Depression Scale of the Depression Anxiety Stress Scales short form (DASS21-DS) is a self report used to examine validity of the HIQ.
Treatment
Traditional treatment of phobias is still in use today. Its underlying theory states that phobic anxiety is conditioned and triggered by a conditional stimulus. By avoiding phobic situation, anxiety is reduced. However, avoidance behaviour is reinforced through negative reinforcement. Wolpe developed a technique called "systematic desensitization to help participants avoid "avoidance". Research results have suggested that even with a decrease in therapeutic contact densensitization is still very effective. However, other studies have shown that therapists play an essential role in acrophobia treatment. Treatments like reinforced practice and self-efficacy treatments also emerged.
There have been a number of studies into using virtual reality therapy for acrophobia. Botella and colleagues and Schneider were the first to use VR in treatment. Specifically, Schneider utilised inverted lenses in binoculars to "alter" the reality. Later in mid 1990s, VR became computer based and was widely available for therapists. A cheap VR equipment uses a normal PC with head-mounted display (HMD). In contrast, VRET uses an advanced computer automatic virtual environment (CAVE). VR has several advantages over in vivo treatment: (1) therapist can control the situation better by manipulating the stimuli, in terms of their quality, intensity, duration and frequency; (2) VR can help participants avoid public embarrassment and protect their confidentiality; (3) therapist's office can be well maintained; (4) VR encourages more people to seek treatment; (5) VR saves time and money as participants do not need to leave the consulting room.
Many different types of medications are used in the treatment of phobias like fear of heights, including traditional anti-anxiety drugs such as benzodiazepines, and newer options like antidepressants and beta-blockers.
Prognosis
Some desensitization treatments produce short-term improvements in symptoms. Long-term treatment success has been elusive.
Epidemiology
True acrophobia is uncommon.
A related, milder form of visually triggered fear or anxiety is called visual height intolerance(vHI). Up to one-third of people may have some level of visual height intolerance. Pure vHI usually has smaller impact on individuals compared to acrophobia, in terms of intensity of syptoms load, social life, and overall life quality. However, only few people with visual height intolerance seek for professional help.
Society and culture
In the Alfred Hitchcock film Vertigo, John "Scottie" Ferguson, played by James Stewart, has to resign from the police force after an incident which causes him to develop both acrophobia and vertigo. The word "vertigo" is only mentioned once, while "acrophobia" is mentioned several times. Early on in the film, Ferguson faints while climbing a step-ladder. There are numerous references throughout the film to fear of heights and falling.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline
#1000 2021-04-25 00:05:49
- Jai Ganesh
- Administrator
- Registered: 2005-06-28
- Posts: 53,807
Re: Miscellany
978) Claustrophobia
Overview
Claustrophobia is a situational phobia triggered by an irrational and intense fear of tight or crowded spaces. It can be triggered by things like being locked in a windowless room, being stuck in a crowded elevator, or driving on a congested highway.
Claustrophobia is one of the most common phobias. If you experience claustrophobia, you may feel like you’re having a panic attack, although claustrophobia isn’t a panic disorder. For some people, claustrophobia may disappear on its own. Others may need therapy to manage and cope with their symptoms.
Symptoms
Symptoms of claustrophobia appear following a trigger for the phobia, such as being in a closed room or a crowded space. What you consider a small space can vary depending on the severity of your phobia.
When experiencing symptoms of claustrophobia, you may feel like you’re having a panic attack. Symptoms of claustrophobia can include:
• sweating
• trembling
• hot flashes
• feeling intense fear or panic
• becoming anxious
• shortness of breath
• hyperventilation
• rapid heartbeat
• chest tightness or pain
• nausea
• feeling faint or lightheaded
• feeling confused or disorientated
These symptoms can be mild or severe. If you’re claustrophobic, you may also:
• avoid triggering situations, such as riding in airplanes, subways, elevators, or in cars during heavy traffic
• automatically and compulsively look for the exits in every space you enter
• feel scared that the doors will shut while you're in a room
• stand near or directly by the exits while in a crowded place
Many situations can trigger claustrophobia. Triggers may include:
• being in a small room without windows
• riding in an airplane or small car
• being in a packed elevator
• undergoing a MRI or CT scan
• standing in a large, but crowded room, like at a party or concert
• standing in a closet
Other places that can trigger claustrophobia include:
• public restrooms
• car washes
• revolving doors
• store dressing rooms
• caves or crawl spaces
• tunnels
Your claustrophobia symptoms may be triggered by other situations not mentioned above. You may also define a small or confined space differently from other people. This is because people have their own unique sense of personal or “near” space. A 2011 study found that people with larger “near” spaces surrounding their body are more likely to feel claustrophobic when that circle is breached. So if your personal space is six feet, and someone is standing four feet away from you, you may begin to panic.
Causes
Little is known about what causes claustrophobia. Environmental factors may play a big part. People typically develop claustrophobia during childhood or in their teenage years.
Claustrophobia could be related to dysfunction of the amygdala, which is the part of the brain that controls how we process fear. The phobia can also be caused by a traumatic event, such as:
• being stuck in a tight or crowded space for an extended period of time
• experiencing turbulence when flying
• being punished by being locked in a small space, like a bathroom
• being stuck on crowded public transportation
• being left in a tight space, like a closet, by accident
You’re also more likely to develop claustrophobia if you grew up with a claustrophobic parent or family member. If a child sees their loved one becoming scared of a small, enclosed space, they may begin to associate fear and anxiety with similar situations.
Diagnosis
You should see a doctor if your symptoms have become persistent. Don’t wait until your claustrophobia becomes too overwhelming. An early diagnosis can help you better manage your symptoms.
Your doctor will review your symptoms and give you a physical exam. They’ll also take into account your history of excessive fear that:
• isn’t associated with another disorder
• may be caused by anticipating an event
• triggers anxiety attacks related to the environment
• disrupts normal every day activities
Treatment
Claustrophobia is most commonly treated by psychotherapy. Different types of counseling can help you overcome your fear and manage your triggers. You should speak with your doctor about what type of therapy will work best for you. Treatment may includeany of the following:
Cognitive behavioral therapy (CBT)
A cognitive behavioral therapist will teach you how to control and alter negative thoughts that arise from situations that trigger your claustrophobia. By learning to change your thoughts, you can learn to change your reaction to these situations.
Rational emotive behavioral therapy (REBT)
REBT is an action-oriented form of CBT that focuses on the present. REBT addresses unhealthy attitudes, emotions, and behaviors. It uses a technique called "disputing" to help people develop realistic and healthy beliefs.
Relaxation and visualization
Therapists will offer different relaxation and visualization techniques to use when you’re in a claustrophobic situation. Techniques may include exercises like counting down from 10 or picturing a safe space. These techniques may help calm your nerves and ease your panic.
Exposure therapy
Exposure therapy is commonly used to treat anxiety disorders and phobias. In this therapy, you’ll be placed in a non-dangerous situation that triggers your claustrophobia in order to confront and overcome your fear. The idea is that the more you’re exposed to what scares you, the less you’ll fear it.
Medication
Your doctor may also prescribe antidepressants or an anti-anxiety medication to help treat your panic and physical symptoms. When prescribed, medications are usually used in addition to therapy.

It appears to me that if one wants to make progress in mathematics, one should study the masters and not the pupils. - Niels Henrik Abel.
Nothing is better than reading and gaining more and more knowledge - Stephen William Hawking.
Offline