Math Is Fun Forum
You are not logged in.
- Topics: Active | Unanswered
#1 This is Cool » CPR (Cardiopulmonary Resuscitation) » Yesterday 18:17:58
- Jai Ganesh
- Replies: 0
Cardiopulmonary Resuscitation (CPR)
Gist
Cardiopulmonary Resuscitation (CPR) is an emergency procedure for someone who is unresponsive and not breathing normally. It involves 30 chest compressions (100-120 per minute) followed by 2 rescue breaths (or continuous "hands-only" compressions) to keep blood flowing to vital organs until professional help arrives.
The 7 steps of CPR (Cardiopulmonary Resuscitation) involve ensuring scene safety, checking responsiveness, calling emergency services, opening the airway, checking for breathing, performing 30 chest compressions, and delivering 2 rescue breaths. These steps are repeated until medical help arrives or the patient wakes up.
Summary
Cardiopulmonary resuscitation (CPR) is an emergency procedure used during cardiac or respiratory arrest that involves chest compressions, often combined with artificial ventilation, to preserve brain function and maintain circulation until spontaneous breathing and heartbeat can be restored. It is recommended for those who are unresponsive with no breathing or abnormal breathing, for example, agonal respirations.
CPR involves chest compressions for adults between 5 cm (2.0 in) and 6 cm (2.4 in) deep and at a rate of at least 100 to 120 per minute. The rescuer may also provide artificial ventilation by either exhaling air into the subject's mouth or nose (mouth-to-mouth resuscitation) or using a device that pushes air into the subject's lungs (mechanical ventilation). Current recommendations emphasize early and high-quality chest compressions over artificial ventilation; a simplified CPR method involving only chest compressions is recommended for untrained rescuers. With children, however, 2015 American Heart Association guidelines indicate that doing only compressions may result in worse outcomes, because such problems in children normally arise from respiratory issues rather than from cardiac ones, given their young age. Chest compression to breathing ratios are set at 30 to 2 in adults.
CPR alone is unlikely to restart the heart. Its main purpose is to restore the partial flow of oxygenated blood to the brain and heart. The objective is to delay tissue death and to extend the brief window of opportunity for a successful resuscitation without permanent brain damage. Administration of an electric shock to the subject's heart, termed defibrillation, is usually needed to restore a viable, or "perfusing", heart rhythm. Defibrillation is effective only for certain heart rhythms, namely ventricular fibrillation or pulseless ventricular tachycardia, rather than asystole or pulseless electrical activity, which usually requires the treatment of underlying conditions to restore cardiac function. Early shock, when appropriate, is recommended. CPR may succeed in inducing a heart rhythm that may be shockable. In general, CPR is continued until the person has a return of spontaneous circulation (ROSC) or is declared dead.
Medical uses
CPR is indicated for any person unresponsive with no breathing or breathing only in occasional agonal gasps, as it is most likely that they are in cardiac arrest. If a person still has a pulse but is not breathing (respiratory arrest), artificial ventilations may be more appropriate, but due to the difficulty people have in accurately assessing the presence or absence of a pulse, CPR guidelines recommend that lay persons should not be instructed to check the pulse while giving healthcare professionals the option to check a pulse. In those with cardiac arrest due to trauma, CPR is considered futile but still recommended. Correcting the underlying cause such as a tension pneumothorax or pericardial tamponade may help.
Details
CPR (cardiopulmonary resuscitation) is an emergency procedure for someone who’s in cardiac arrest. CPR with breaths and hands-only CPR are the two types. Even if you’re not CPR-certified, you can do hands-only CPR. This involves doing 100 to 120 chest compressions per minute. Start CPR immediately to give the person the best chance of survival.
What Is CPR?
CPR stands for cardiopulmonary resuscitation. It’s an emergency procedure that can save your life if you’re in cardiac arrest. This means your heart stops beating and can’t pump blood out to your body. The key part of CPR is chest compressions (pushing hard and fast in the center of the chest). This keeps some blood flowing to vital organs. CPR may also involve mouth-to-mouth breaths, which give you oxygen.
Healthcare providers, like doctors, nurses and paramedics, routinely perform CPR both in and out of hospitals. Others, called lay rescuers, can also perform CPR wherever it’s needed, like at homes, gyms and shopping malls.
If you’re reading this and aren’t a healthcare provider, you have the opportunity to be a lay rescuer. This means you can save someone’s life, no matter who you are. Lay rescuers include people with CPR certification (you take classes and get an official certificate), as well as those without it. You’ll do the type of CPR that reflects your training and comfort level.
Types of CPR
There are two main types of CPR:
* CPR with breaths (conventional CPR): You use chest compressions and mouth-to-mouth breaths. You need CPR certification to do this type.
* Hands-only CPR: You only use chest compressions (no breaths). You don’t need CPR certification to do this type. You can learn on your own.
Both types are effective and can be lifesaving within the first few minutes of cardiac arrest in adults. However, CPR with breaths is more helpful in situations where CPR must go on for longer than a few minutes. This is because the person’s blood needs more oxygen at that point to prevent damage to vital organs like the brain.
How to recognize when someone needs CPR
A person needs CPR if they’re unconscious and have absent or abnormal breathing. Here’s what that means:
* Unconscious: This is also called being “unresponsive.” It means the person doesn’t respond if you shout, say their name or tap them on the shoulder.
* Absent or abnormal breathing: This means the person either isn’t breathing, or they’re breathing in ways that don’t sound normal. It may sound like they’re gasping for air.
These are signs that the person is in cardiac arrest.
What not to do
When someone’s in cardiac arrest, do NOT delay CPR in order to:
* Check for a pulse: The latest guidelines say that lay rescuers should NOT check for a pulse (this is true even if you’re CPR certified). This can waste valuable time. If the person is unresponsive and not breathing right, start CPR right away.
* Check their airways for an object that’s stuck: The guidelines do NOT recommend routine inspection of the mouth or throat when a person is in cardiac arrest. Also, never do a “blind finger sweep,” looking for an object. This can push any object deeper into the airway.
The only time to check the airways for a lodged object is if you witness someone collapse while choking. In that case, quickly look in their mouth. Don’t feel around for an object. But if you can clearly see an object and it’s easily removed, you can remove it. Otherwise, start CPR right away.
Procedure Details
Before starting CPR, quickly ask someone to:
* Call your local emergency services number): Ideally, someone nearby can make the call so you can immediately start CPR. But if you’re alone, call for emergency help and put the phone on speaker while you get started.
8 Get an automated external defibrillator (AED): An AED is a device that can restart the heart. AEDs are available in many public places. You can use them even if you don’t have training. The device will give you instructions aloud.
It may take some minutes for emergency services to arrive and for someone to find an AED. Don’t wait. Start CPR immediately.
CPR steps for adults and teens
1. Make sure the person is on a firm, flat surface. They should be lying on their back. Gently position the person as needed.
2. Kneel down. You should be next to the person, with your knees about shoulder width apart.
3. Place your hands on their chest. Put the heel of one hand in the middle of their chest, with your fingers lifted upward and spread out. Put your other hand on top and interlace your fingers. Your fingers should be slightly lifted up off their chest, with the lower heel pressing down.
4. Position your body. Your shoulders should be directly over your hands. Your arms should extend straight downward, with your elbows locked (not bent). This helps you use your body weight to push down forcefully enough.
5. Start chest compressions. Push down on the middle of the person’s chest with hard, fast movements. Their chest should go down by at least 2 inches (5 centimeters) each time, but not more than 2.4 inches (6 centimeters). Their chest should rise up before you push again.
6. Keep a steady pace. Do chest compressions at a rate of 100 to 120 per minute. This follows the beat of “Stayin’ Alive,” by the Bee Gees, and “Crazy in Love,” by Beyoncé and Jay-Z. Make sure you allow the person’s chest to come all the way back up between compressions.
7. Give breaths (IF TRAINED). For hands-only CPR, simply continue doing chest compressions. But if you’re CPR certified and willing to give breaths, you should do so. Follow the guidance you learned in your training. You should generally give two breaths after every 30 compressions.
Continue doing CPR until any of the following happen:
* The person starts breathing normally again.
* First responders arrive and take over the care.
* An AED is available to use (if this happens, stop CPR and start using the AED right away).
If at any point, you feel too tired to continue, let someone else who’s ready step in. Make the switch as quickly as possible so there aren’t long breaks in between compressions. Generally, it’s advised to switch personnel every two minutes.
CPR steps for children and babies
There are some key differences when you’re doing CPR for anyone 12 or younger. Here’s what to know:
* CPR with breaths is best for children and babies. This means, ideally, someone who’s CPR certified will step in. But if no one with training is available, it’s OK to do hands-only CPR.
* For infants, don’t use both hands for chest compressions. Instead, use modified techniques that are more appropriate for an infant’s small size. These are described farther below. The infant’s chest should go down by about 1.5 inches (4 centimeters).
* For children, use either one or two hands for chest compressions. It depends on the size of the child. For children 1 to 8 years old, using one hand may be OK as long as you can keep the proper form. The child’s chest should go down by about 2 inches (5 centimeters).
When performing CPR on an infant (1 to 12 months old), use one of the following techniques for chest compressions:
* The “two thumb-encircling hands” technique: You wrap both hands around the infant’s upper body. Your thumbs should meet at the center of their chest, forming an upside-down V. Push down with both thumbs. This is better than doing two-finger compressions (an older method).
* The “heel-of-one-hand” technique: If you can’t wrap both hands around the infant, then use the heel of one hand (not both) to do chest compressions.
What are the potential benefits and risks of CPR?
CPR can save your life if you receive it right after going into cardiac arrest. CPR keeps blood moving through your body. This may prevent organ damage, like cerebral hypoxia.
Some people with certain preexisting health conditions might not experience the same benefits from CPR. It depends on how sick you are before you go into cardiac arrest. Consider speaking with a healthcare provider you trust about what your recovery or outlook might look like if you needed CPR.
Possible risks of CPR include broken ribs and injury to organs in your chest. This is because chest compressions must be forceful to keep blood circulating and keep you alive.
Recovery and Outlook:
What happens immediately after CPR?
If you’re a lay rescuer, you’ll step back when first responders arrive. They’ll take over and begin providing medical care. They’ll transport the person to a hospital as soon as possible. If the person survives, healthcare providers will check for any organ damage from a lack of oxygen. They’ll also determine the cause of cardiac arrest and provide any needed treatment.
If a cardiac arrest occurs at home and an individual wakes up after CPR from a non-trained family member, they should be evaluated immediately by a healthcare team. This is true even if they look well.
Additional Information
CPR stands for cardiopulmonary resuscitation. It can help save a life during cardiac arrest, when the heart stops beating or beats too ineffectively to circulate blood to the brain and other vital organs.
What Is the Purpose of CPR?
With a half-million cardiac arrests each year, CPR increases the likelihood of surviving cardiac arrest, when the heart stops beating or beats too ineffectively to circulate blood to the brain and other vital organs. It’s not just for healthcare workers and emergency responders. CPR can double or triple the chance of survival when bystanders take action. The Red Cross helps train you safely, effectively and confidently so you’re prepared for the moments that matter.
Why is CPR Important?
CPR should be used when you see someone who is unresponsive and is not breathing or only gasping. Having more bystanders trained in this simple skill can help save lives by putting more cardiac arrest victims within a few steps of lifesaving assistance.
What Are the Types of CPR?
* Hands-Only CPR: Hands-only CPR is an easy-to-learn skill that could save a life. It involves calling 9-1-1, sending someone for the AED if available and then giving continuous chest compressions. It only takes minutes to learn.
* Full CPR With Rescue Breaths: While Hands-only CPR can be lifesaving, learning full CPR is still very important. Getting trained in full CPR – combinations of chest compressions and rescue breaths – will increase your confidence and may enable you to help in other types of emergencies. Full CPR is ideal for all ages, and especially for people who are more likely to experience respiratory emergencies such as children and infants.
Why Learn CPR?
Learning how to perform CPR properly takes just a few short hours, but it can change a life forever. Red Cross CPR training classes give you the information and the skills you need to help adults, children and infants during cardiac emergencies. Whether you choose 100% in-person or blended learning CPR classes, our world-class instructors deliver the most up-to-date information that's engaging and effective, preparing you for the moments that matter.
Benefits to Being CPR Certified
* An Emergency Can Happen When You Least Expect It. No one ever expects emergencies to occur as they go about their day, which is why it is important to learn CPR ahead of time. Cardiac arrest can happen at home, at school, at the gym, on an airplane, in the workplace or anywhere in the community. CPR is a critical skill that can help save a life when a person's breathing or heart stops.
* Every Second Counts. You may be wondering, "why learn CPR when I can just call 9-1-1?" While you should always call 9-1-1 first in the event of an emergency, it still takes rescuers some time to arrive at the scene. For every minute without intervention, the chance of survival drops for a person experiencing sudden cardiac arrest. CPR can significantly improve someone’s chance of surviving when bystanders take prompt action.
* CPR Also Prevents Brain Death. Even if someone survives cardiac arrest, they may suffer permanent brain damage when they don't receive enough blood flow and oxygen to the brain. CPR certification can help prevent brain damage and death by keeping oxygenated blood moving throughout the body.
* Anyone Can Learn It. Another benefit of CPR is that this lifesaving training is for everyone. It only takes a few hours, and it can give you the skills and confidence to act in an emergency and help save a life. You'll find classes that are designed for the way you live and learn, with options available on weekdays and weekends in a variety of formats.
* You'll Have the Confidence to Act when Needed. CPR instruction will give you the skills and confidence to perform this life-saving procedure when it's needed the most. Plus, to keep your skills fresh, online refresher materials are available that can help you retain the knowledge you've gained. In addition, you'll also have access to a printable list of the basic steps for performing CPR. This way, you can keep the information you need right at your fingertips.
Cardiac Arrest Chain of Survival
Cardiac arrest can happen anytime and anywhere. In these emergencies, the heart stops beating or beats too ineffectively to circulate blood to the brain and other vital organs. The cardiac arrest out-of-hospital chain of survival shows the steps necessary to take in order to improve chances of survival from cardiac arrest.
The 6 links in the adult out-of-hospital Chain of Survival are:
* Recognition of cardiac arrest and activation of the emergency response system (such as calling 9-1-1)
* Early CPR with an emphasis on chest compressions
* Rapid defibrillation
* Advanced resuscitation by Emergency Medical Services (EMS) and other healthcare providers
* Post-cardiac arrest care in the hospital
* Recovery (such as additional treatment, rehabilitation, and psychological support)
CPR/AED Classes
At the Red Cross, you can choose the type of class for your schedule – and the way you learn best. For those who want to become certified in CPR/AED, you can choose from three types of courses:
* In-person: Designed for those who learn best in a traditional classroom setting, our in-person courses combine lecture with hands-on skills sessions. This way, you can not only learn what CPR is, but you will be able to practice your skills with a certified instructor. If the course is completed with a passing grade, you'll receive a two-year certification.
* Online: Perfect for those who want the freedom to take self-paced courses, our online classes can help you learn what CPR is and how to perform the different types of CPR. However, online safety training courses do not allow you to demonstrate your skill proficiency to a certified instructor, and therefore your certification may not meet the requirements for workplace safety.
* Blended Learning: Our blended learning programs combine self-paced, interactive instruction and in-person skills sessions. That way, you can learn what CPR is, why CPR is important and how to perform it in theory and in practice. Additionally, because this option allows you to demonstrate your skills to a certified instructor, you can receive full certification with a passing score.

#2 Science HQ » Duodenum » Yesterday 16:48:34
- Jai Ganesh
- Replies: 0
Duodenum
Gist
The duodenum is the first, shortest (approx. 25–30 cm), and most fixed "C"-shaped section of the small intestine, connecting the stomach to the jejunum. It neutralizes acidic chyme and breaks down fats, proteins, and carbohydrates using bile and pancreatic enzymes, playing a critical role in nutrient absorption.
What is the main function of the duodenum?
The first part of the small intestine. It connects to the stomach. The duodenum helps to further digest food coming from the stomach. It absorbs nutrients (vitamins, minerals, carbohydrates, fats, proteins) and water from food so they can be used by the body.
Summary
The duodenum is the first section of the small intestine in most vertebrates, including mammals, reptiles, and birds. In mammals, it may be the principal site for iron absorption. The duodenum precedes the jejunum and ileum and is the shortest part of the small intestine.
In humans, the duodenum is a hollow jointed tube about 25–38 centimetres (10–15 inches) long connecting the stomach to the jejunum, the middle part of the small intestine. It begins with the duodenal bulb, and ends at the duodenojejunal flexure marked by the suspensory muscle of duodenum. The duodenum can be divided into four parts: the first (superior), the second (descending), the third (transverse) and the fourth (ascending) parts.
Overview
The duodenum is the first section of the small intestine in most higher vertebrates, including mammals, reptiles, and birds. In fish, the divisions of the small intestine are not as clear, and the terms anterior intestine or proximal intestine may be used instead of duodenum. In mammals the duodenum may be the principal site for iron absorption.
In humans, the duodenum is a C-shaped hollow jointed tube, 25–38 centimetres (10–15 inches) in length, lying adjacent to the stomach (and connecting it to the small intestine). It is divided anatomically into four sections. The first part lies within the peritoneum but its other parts are retroperitoneal.
Details
The duodenum is the first part of your small intestine. Its main job is to transform the partially digested food it receives from your stomach into nutrients your body can use. Digestive juices from your liver, gallbladder and pancreas empty into your duodenum, helping with digestion and absorption.
Overview:
What is the duodenum?
The duodenum is the first part of your small intestine. Despite what the name suggests, your “small” intestine is the longest part of your digestive tract and plays a big role in your digestive system. Inside its many coils, digestive juices transform food into the nutrients (like proteins, fats, vitamins and water) that power your body.
The duodenum is a short, “C”-shaped chute. It’s the first stop food makes as it travels from your stomach to your small intestine. The other parts of your small intestine are your jejunum (the middle part) and ileum (the last part).
Function:
What is the function of the duodenum?
The duodenum continues the process of digestion (breakdown of food into nutrients) that starts in other parts of your gastrointestinal (GI) tract, like your mouth and stomach. It also begins the absorption process (moving the nutrients into your bloodstream). Think of it this way: Before reaching your duodenum, saliva and stomach acid have transformed food into food slush. Inside your duodenum, the slush becomes nutrients your body can use.
Your duodenum:
* Makes food traveling from your stomach less acidic. The partially digested food that travels from your stomach to your duodenum is called chyme. Chyme is highly acidic, thanks to stomach juices that break down food. Your duodenum releases a hormone (secretin) that triggers the release of an enzyme called bicarbonate that makes chyme less acidic. The breakdown of acid helps your digestive system absorb nutrients. It prevents the acid from damaging your small intestine.
* Transforms chyme into nutrients. Your duodenum releases a hormone (cholecystokinin) that triggers your pancreas, gallbladder and liver to release substances that help turn chyme into nutrients. Your liver and gallbladder release bile, which breaks down fats. Your pancreas releases lipase, which also breaks down fats, amylase to break down carbohydrates and protease to break down proteins. Your bloodstream absorbs these nutrients.
* Moves food molecules along. The duodenum pushes food molecules that don’t get absorbed into the next section of your small intestine, the jejunum. The duodenum squeezes and relaxes, creating a wave-like forward motion called peristalsis.
Anatomy:
How big is the duodenum?
It’s the shortest section of your small intestine, approximately 10 inches long — just 2 inches shy of a foot. “Duodenum,” translated from Latin, means “12 fingers,” a reference to its size. The length of your duodenum is approximately the width of 12 fingers placed side by side.
To put this in perspective, your entire small intestine is 22 feet long. If you stretched it out, it would be the length of a tennis court. Your duodenum wouldn’t be a single foot of the total length. Yet, important nutrient absorption happens in these 10 inches of your small intestine.
Where is the duodenum located?
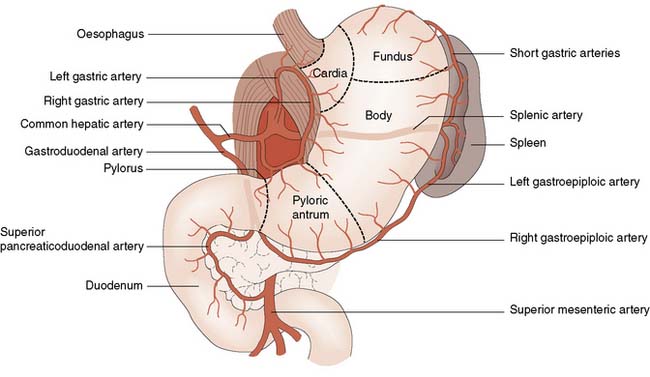
Your duodenum starts just below your stomach. It curves to the right and back, down and then to the left in a “C” or horseshoe shape. It slants upward slightly before joining with the next part of your small intestine, your jejunum. The head of your pancreas (the widest part) sits inside the “C.”
What are the parts of the duodenum?
There are four basic parts. They get their name from their location and shape.
* Superior segment
The superior segment is the top part of the duodenum that connects with your stomach. It’s about 2 inches long. The part of the superior segment that connects directly with your pylorus (the stomach valve that opens to allow food to travel to your small intestine) is called the duodenal bulb. Most ulcers in your small intestine form here, where stomach acid is most likely to come into contact with your duodenum.
* Descending segment
As the name suggests, the descending segment is the part of the “C” shape that goes downward. It passes in front of your right kidney and is about 4 inches long.
This part of your small intestine connects to your pancreas (via the pancreatic duct) and your gallbladder and liver (via the common bile duct). “Ducts” are like tiny canals that allow substances to travel from one organ (like your liver) to another organ (like your small intestine). These organs produce substances that empty into the descending segment, breaking down fats, proteins and carbohydrates.
* Horizontal (inferior) segment
The horizontal segment is about 4 inches long. It extends from right to left and passes over essential blood vessels, including your aorta and inferior vena cava.
* Ascending segment
This is the smallest part of your duodenum, at just under an inch. It extends slightly upward and is located to the left of your aorta. It connects to your jejunum.
What is the duodenum made of?
The duodenum has four layers. Its cell makeup is the same as other organs in your GI tract. From the innermost layer to the outermost layer, the duodenum consists of the:
* Mucosa: It contains glands and fingerlike projections called microvilli. The microvilli increase the surface area of your duodenum, allowing it to absorb more nutrients than if it were flat.
* Submucosa: This layer consists of blood vessels and connective tissue. The submucosa contains Brunner’s glands. Brunner’s glands release a substance that makes chyme less acidic.
* Muscularis: This layer is mostly smooth muscle. Its job is mixing and moving. As it contracts, it blends the enzymes and bile that break down chyme. It also moves the chyme along the length of your duodenum, so it reaches your jejunum.
* Serosa: This layer consists of squamous epithelial cells that serve as your duodenum’s protective barrier.
Conditions and Disorders:
What problems can occur in the duodenum?
As the part of your small intestine closest to your stomach, your duodenum is especially susceptible to injury if you have excess stomach acid. The acid can lead to open stores in your stomach (peptic ulcers) and in your duodenum. The most common causes of these ulcers are H. pylori infection and overusing medicines called NSAIDs (nonsteroidal anti-inflammatory drugs). NSAIDs, like aspirin and ibuprofen, can ease symptoms like aches and pains but can cause ulcers if you use them too much.
If an untreated ulcer breaks down too much of your duodenum’s protective barrier, its contents can leak out and damage the gastroduodenal artery behind it. This can cause severe bleeding that requires emergency care.
Many of the same conditions that affect your small intestine, in general, can affect your duodenum specifically. Conditions that can affect your duodenum include:
* Brunner’s gland adenomas: Benign (noncancerous) growths that start in Brunner’s glands.
* Crohn’s disease: A type of irritable bowel disease (IBD) that causes irritation and inflammation.
* Celiac disease: A disorder that causes problems in your digestive system when you eat gluten.
* Duodenal atresia: A condition that causes a baby to be born with a closed duodenum.
* Duodenal stenosis: A condition that causes a baby to be born with a narrowed (but not completely closed) duodenum.
* Duodenal cancer: Cancer that starts in your duodenum.
* Duodenal diverticulum: A small, pouch-like structure that pushes outside the wall of your duodenum. Diverticula (plural of diverticulum) usually don’t cause issues or require treatment unless they become infected and inflamed (diverticulitis).
* Duodenitis: Inflammation in your duodenum.
* Small bowel obstruction: A medical emergency that happens when part of your small intestine (including your duodenum) is entirely or partially blocked.
Common signs or symptoms of issues with the duodenum
Symptoms depend on the specific condition. In general, symptoms of a condition affecting your duodenum are similar to problems with your GI tract. Signs and symptoms include:
* Abdominal pain.
* Bloating and gas.
* Constipation.
* Diarrhea.
* Nausea and vomiting.
* Indigestion (stomach discomfort after you eat).
* Bloody vomit or poop (a sign of a bleeding ulcer).
Common tests to check the health of the duodenum.
Common tests include:
* Breath test to check for H. pylori infections.
* Imaging procedures — like ultrasounds, X-rays, CT scans (computed tomography scans) and MRIs (magnetic resonance imaging) — that look for growths and inflammation inside your duodenum.
* Procedures that use a scope to see inside your duodenum, including enteroscopy and upper endoscopy.
* Biopsies to check abnormal growths, including cancer.
What are common treatments for conditions affecting the duodenum?
Common treatments include:
* Antibiotics to treat infections (like H. pylori).
* Corticosteroids to reduce severe inflammation.
* Medicines to reduce the amount or acidity level of stomach acid, like proton pump inhibitors (PPIs), histamine receptor blockers (H2 blockers) and antacids.
* Surgery to correct structural issues or treat cancer, including the Whipple procedure.
Care:
How can I keep my duodenum healthy?
Putting healthy habits into place to prevent irritating or overworking your digestive system is good for your entire GI tract, including your duodenum.
Choose a diet that keeps your digestive system running smoothly. Eating lots of fiber and drinking lots of water can help you have regular bowel movements so things don’t get backed up in your small intestine. Eating lots of vegetables and nonacidic foods can help you maintain a healthy acidity level in your gut.
Avoid substances that can irritate your gut. Smoking and drinking too much alcohol can irritate organs in your digestive system, including your small intestine. Taking too many NSAIDs (Nonsteroidal anti-inflammatory drugs) can lead to painful ulcers that require treatment.
Don’t ignore signs of digestive system issues. Changes in your bowel habits and unpleasant symptoms, like an upset stomach or indigestion, can be temporary. Or they can sound the alarm bells that you need to change your lifestyle or see a provider. Don’t delay getting help if you’ve got unpleasant digestive symptoms that aren’t improving.
Additional Information
Duodenum is the first part of the small intestine, which receives partially digested food from the stomach and begins the absorption of nutrients. The duodenum is the shortest segment of the intestine and is about 23 to 28 cm (9 to 11 inches) long. It is roughly horseshoe-shaped, with the open end up and to the left, and it lies behind the liver. On anatomic and functional grounds, the duodenum can be divided into four segments: the superior (duodenal bulb), descending, horizontal, and ascending duodenum.
A liquid mixture of food and gastric secretions enters the superior duodenum from the pylorus of the stomach, triggering the release of pancreas-stimulating hormones (e.g., secretin) from glands (crypts of Lieberkühn) in the duodenal wall. So-called Brunner glands in the superior segment provide additional secretions that help to lubricate and protect the mucosal layer of the small intestine. Ducts from the pancreas and gallbladder enter at the major duodenal papilla (papilla of Vater) in the descending duodenum, bringing bicarbonate to neutralize the acid in the gastric secretions, pancreatic enzymes to further digestion, and bile salts to emulsify fat. A separate minor duodenal papilla, also in the descending segment, may receive pancreatic secretions in small amounts. The mucous lining of the last two segments of the duodenum begins the absorption of nutrients, in particular iron and calcium, before the food contents enter the next part of the small intestine, the jejunum.
Inflammation of the duodenum is known as duodenitis, which has various causes, prominent among them infection by the bacterium Helicobacter pylori. H. pylori increases the susceptibility of the duodenal mucosa to damage from unneutralized digestive acids and is a major cause of peptic ulcers, the most common health problem affecting the duodenum. Other conditions that may be associated with duodenitis include celiac disease, Crohn disease, and Whipple disease. The horizontal duodenum, because of its location between the liver, pancreas, and major blood vessels, can become compressed by those structures in people who are severely thin, requiring surgical release to eliminate painful duodenal dilatation, nausea, and vomiting.
#3 Re: Jai Ganesh's Puzzles » General Quiz » Yesterday 15:47:55
Hi,
#10809. What does the term in Geography Discordant coastline mean?
#10810. What does the term in Geography Dissected plateau mean?
#4 Re: Jai Ganesh's Puzzles » English language puzzles » Yesterday 15:31:29
Hi,
#6015. What does the adjective lucrative mean?
#6016. What does the noun luge mean?
#5 Re: Jai Ganesh's Puzzles » Doc, Doc! » Yesterday 15:16:12
Hi,
#2604. What does the medical term Heartburn mean?
#6 Re: Jai Ganesh's Puzzles » 10 second questions » Yesterday 15:06:23
Hi,
#9890.
#7 Re: Jai Ganesh's Puzzles » Oral puzzles » Yesterday 14:34:48
Hi,
#6383.
#8 Re: Exercises » Compute the solution: » Yesterday 13:59:00
Hi,
2744.
#9 Re: This is Cool » Miscellany » Yesterday 00:49:35
2530) Amphibian
Gist
Amphibians are cold-blooded, vertebrate animals (possessing a backbone) that inhabit both aquatic and terrestrial environments. The name derives from Greek, meaning "living a double life" because they typically undergo metamorphosis, starting life in water with gills and developing lungs for land-based adult life.
The word amphibian was taken from the Greek “amphi” meaning “double” and “bios” meaning “life” which is quite fitting as these creatures do live a double life. Emerging from eggs that are usually laid in the water, most amphibians begin their life with gills.
Summary
Amphibians are ectothermic, anamniotic, four-limbed vertebrate animals that constitute the class Amphibia. In its broadest sense, it is a paraphyletic group encompassing all tetrapods, but excluding the amniotes (tetrapods with an amniotic membrane, such as modern reptiles, birds and mammals). All extant (living) amphibians belong to the monophyletic subclass Lissamphibia, with three living orders: Anura (frogs and toads), Urodela (salamanders), and Gymnophiona (caecilians). Evolved to be mostly semiaquatic, amphibians have adapted to inhabit a wide variety of habitats, with most species living in freshwater, wetland or terrestrial ecosystems (such as riparian woodland, fossorial and even arboreal habitats). Their life cycle typically starts out as aquatic larvae with gills known as tadpoles, but some species have developed behavioural adaptations to bypass this.
Young amphibians generally undergo metamorphosis from an aquatic larval form with gills to an air-breathing adult form with lungs. Amphibians use their skin as a secondary respiratory interface, and some small terrestrial salamanders and frogs even lack lungs and rely entirely on their skin. They are superficially similar to reptiles like lizards, but unlike reptiles and other amniotes, require access to water bodies to breed. With their complex reproductive needs and permeable skins, amphibians are often ecological indicators to habitat conditions; in recent decades there has been a dramatic decline in amphibian populations for many species around the globe.
The earliest amphibians evolved in the Devonian period from tetrapodomorph sarcopterygians (lobe-finned fish with articulated limb-like fins) that evolved primitive lungs, which were helpful in adapting to dry land. They diversified and became ecologically dominant during the Carboniferous and Permian periods, but were later displaced in terrestrial environments by early reptiles and basal synapsids (predecessors of mammals). The origin of modern lissamphibians, which first appeared during the Early Triassic, around 250 million years ago, has long been contentious. The most popular hypothesis is that they likely originated from temnospondyls, the most diverse group of prehistoric amphibians, during the Permian period. Another hypothesis is that they emerged from lepospondyls. A fourth group of lissamphibians, the Albanerpetontidae, became extinct around 2 million years ago.
The number of known amphibian species is approximately 8,000, of which nearly 90% are frogs. The smallest amphibian (and vertebrate) in the world is a frog from New Guinea (Paedophryne amauensis) with a length of just 7.7 mm (0.30 in). The largest living amphibian is the 1.8 m (5 ft 11 in) South China giant salamander (Andrias sligoi), but this is dwarfed by prehistoric temnospondyls such as Mastodonsaurus which could reach up to 6 m (20 ft) in length. The study of amphibians is called batrachology, while the study of both reptiles and amphibians is called herpetology.
Details
An amphibian is (class Amphibia), any member of the group of vertebrate animals characterized by their ability to exploit both aquatic and terrestrial habitats. The name amphibian, derived from the Greek amphibios meaning “living a double life,” reflects this dual life strategy—though some species are permanent land dwellers, while other species have a completely aquatic mode of existence.
Approximately 8,100 species of living amphibians are known. First appearing about 340 million years ago during the Middle Mississippian Epoch, they were one of the earliest groups to diverge from ancestral fish-tetrapod stock during the evolution of animals from strictly aquatic forms to terrestrial types. Today amphibians are represented by frogs and toads (order Anura), newts and salamanders (order Caudata), and caecilians (order Gymnophiona). These three orders of living amphibians are thought to derive from a single radiation of ancient amphibians, and although strikingly different in body form, they are probably the closest relatives to one another. As a group, the three orders make up subclass Lissamphibia. Neither the lissamphibians nor any of the extinct groups of amphibians were the ancestors of the group of tetrapods that gave rise to reptiles. Though some aspects of the biology and anatomy of the various amphibian groups might demonstrate features possessed by reptilian ancestors, amphibians are not the intermediate step in the evolution of reptiles from fishes.
Modern amphibians are united by several unique traits. They typically have a moist skin and rely heavily on cutaneous (skin-surface) respiration. They possess a double-channeled hearing system, green rods in their retinas to discriminate hues, and pedicellate (two-part) teeth. Some of these traits may have also existed in extinct groups.
Members of the three extant orders differ markedly in their structural appearance. Frogs and toads are tailless and somewhat squat with long, powerful hind limbs modified for leaping. In contrast, caecilians are limbless, wormlike, and highly adapted for a burrowing existence. Salamanders and newts have tails and two pairs of limbs of roughly the same size; however, they are somewhat less specialized in body form than the other two orders.
Many amphibians are obligate breeders in standing water. Eggs are laid in water, and the developing larvae are essentially free-living embryos; they must find their own food, escape predators, and perform other life functions while they continue to develop. As the larvae complete their embryonic development, they adopt an adult body plan that allows them to leave aquatic habitats for terrestrial ones. Even though this metamorphosis from aquatic to terrestrial life occurs in members of all three amphibian groups, there are many variants, and some taxa bear their young alive. Indeed, the roughly 8,100 living species of amphibians display more evolutionary experiments in reproductive mode than any other vertebrate group. Some taxa have aquatic eggs and larvae, whereas others embed their eggs in the skin on the back of the female; these eggs hatch as tadpoles or miniature frogs. In other groups, the young develop within the oviduct, with the embryos feeding on the wall of the oviduct. In some species, eggs develop within the female’s stomach.
The three living orders of amphibians vary greatly in size and structure. The presence of a long tail and two pairs of limbs of about equal size distinguishes newts and salamanders (order Caudata) from other amphibians, although members of the eel-like family Sirenidae have no hind limbs. Newts and salamanders vary greatly in length; members of the Mexican genus Thorius measure 25 to 30 mm (1 to 1.2 inches), whereas Andrias, a genus of giant aquatic salamanders endemic to China and Japan, reaches a length of more than 1.5 metres (5 feet). Frogs and toads (order Anura) are easily identified by their long hind limbs and the absence of a tail. They have only five to nine presacral vertebrae. The West African goliath frog, which can reach 30 cm (12 inches) from snout to vent and weigh up to 3.3 kg (7.3 pounds), is the largest anuran. Some of the smallest anurans include the South American brachycephalids, which have an adult snout-to-vent length of only 9.8 mm (0.4 inch), and some microhylids, which grow to 9 to 12 mm (0.4 to 0.5 inch) as adults. The long, slender, limbless caecilians (order Gymnophiona) are animals that have adapted to fossorial (burrowing) lifestyles by evolving a body segmented by annular grooves and a short, blunt tail. Caecilians can grow to more than 1 metre (3 feet) long. The largest species, Caecilia thompsoni, reaches a length of 1.5 metres (5 feet), whereas the smallest species, Idiocranium russeli, is only 90 to 114 mm (3.5 to 5 inches) long.
Distribution and abundance
Amphibians occur widely throughout the world, even edging north of the Arctic circle in Eurasia; they are absent only in Antarctica, most remote oceanic islands, and extremely xeric (dry) deserts. Frogs and toads show the greatest diversity in humid tropical environments. Salamanders primarily inhabit the Northern Hemisphere and are most abundant in cool, moist, montane forests; however, members of the family Plethodontidae, the lungless salamanders, are diverse in the humid tropical montane forests of Mexico, Central America, and northwestern South America. Caecilians are found spottily throughout the African, American, and Asian wet tropics.
For many years, habitat destruction has had a severe impact on the distribution and abundance of numerous amphibian species. Since the 1980s, a severe decline in the populations of many frog species has been observed. Although acid rain, global warming, and ozone depletion are contributing factors to these reductions, a full explanation of the disappearance in diverse environment remains uncertain. A parasitic fungus, the so-called amphibian chytrid (Batrachochytrium dendrobatidis), however, appears to be a major cause of substantial frog die-offs in parts of Australia and southern Central America and milder events in North America and Europe.
Economic importance
Amphibians, especially anurans, are economically useful in reducing the number of insects that destroy crops or transmit diseases. Frogs are exploited as food, both for local consumption and commercially for export, with thousands of tons of frog legs harvested annually. The skin secretions of various tropical anurans are known to have hallucinogenic effects and effects on the central nervous and respiratory systems in humans. Some secretions have been found to contain magainin, a substance that provides a natural antibiotic effect. Other skin secretions, especially toxins, have potential use as anesthetics and painkillers. Biochemists are currently investigating these substances for medicinal use.
Natural history:
Reproduction
The three living groups of amphibians have distinct evolutionary lineages and exhibit a diverse range of life histories. The breeding behaviour of each group is outlined below. One similar tendency among amphibians has been the evolution of direct development, in which the aquatic egg and free-swimming larval stages are eliminated. Development occurs fully within the egg capsule, and juveniles hatch as miniatures of the adult body form. Most species of lungless salamanders (family Plethodontidae), the largest salamander family, some caecilians, and many species of anurans have direct development. In addition, numerous caecilians and a few species of anurans and salamanders give birth to live young (viviparity).
Anurans display a wide variety of life histories. Centrolenids and phyllomedusine hylids deposit eggs on vegetation above streams or ponds; upon hatching, the tadpoles (anuran larvae) drop into the water where they continue to develop throughout their larval stage. Some species from the families Leptodactylidae and Rhacophoridae create foam nests for their eggs in aquatic, terrestrial, or arboreal habitats; after hatching, tadpoles of these families usually develop in water. Dendrobatids and other anurans deposit their eggs on land and transport them to water. Female hylid marsupial frogs are so called because they carry their eggs in a pouch on their backs. A few species lack a pouch and the tadpoles are exposed on the back; in some species, the female deposits her tadpoles in a pond as soon as they emerge.
Embryonic stage
Inside the egg, the embryo is enclosed in a series of semipermeable gelatinous capsules and suspended in perivitelline fluid, a fluid that also surrounds the yolk. The hatching larvae dissolve these capsules with enzymes secreted from glands on the tips of their snouts. The original yolk mass of the egg provides all nutrients necessary for development; however, various developmental stages utilize different nutrients. In early development, fats are the major energy source. During gastrulation, an early developmental stage in which the embryo consists of two cell layers, there is an increasing reliance on carbohydrates. After gastrulation, a return to fat utilization occurs. During the later developmental stages, when morphological structures form, proteins are the primary energy source. By the neurula stage, an embryonic stage in which nervous tissue develops, cilia appear on the embryo, and the graceful movement of these hairlike structures rotates the embryo within the perivitelline fluid. The larvae of direct developing and live-bearing caecilians, salamanders, and some anurans have external gills that press against the inner wall of the egg capsule, which permits an exchange of gases (oxygen and carbon dioxide) with the outside air or with maternal tissues. During development, ammonia is the principal form of nitrogenous waste, and it is diluted by a constant diffusion of water in the perivitelline fluid.
The development of limbs in the embryos of aquatic salamanders begins in the head region and proceeds in a wave down the body, and digits appear sequentially on both sets of limbs. Salamanders that deposit their eggs in streams produce embryos that develop both sets of limbs before they hatch, but salamanders that deposit their eggs in still water have embryos that develop only forelimbs before hatching. (In contrast, the limbs of anurans do not appear until after hatching.) Soon after the appearance of forelimbs, most pond-dwelling salamanders develop an ectodermal projection known as a balancer on each side of the head. These rodlike structures arise from the mandibular arch, contain nerves and capillaries, and produce a sticky secretion. They keep newly hatched larvae from sinking into the sediment and aid the salamander in maintaining its balance before its forelimbs develop. After the forelimbs appear, the balancers degenerate.
During the embryonic and early larval stages in anurans, paired adhesive organs arise from the hyoid arch, located at the base of the tongue. The sticky mucus they secrete can form a threadlike attachment between a newly hatched tadpole and the egg capsule or vegetation. Consequently, the tadpole that is still developing can remain in a stable position until it is capable of swimming and feeding on its own, after which the adhesive organs degenerate.
Larval stage
The amphibian larva represents a morphologically distinct stage between the embryo and adult. The larva is a free-living embryo. It must find food, avoid predators, and participate in all other aspects of free-living existence while it completes its embryonic development and growth. Salamander and caecilian larvae are carnivorous, and they have a morphology more like their respective adult forms than do anuran larvae. Not long after emerging from their egg capsules, larval salamanders, which have four fully developed limbs, start to feed on small aquatic invertebrates. The salamander larvae are smaller versions of adults, although they differ from their adult counterparts by the presence of external gills, a tailfin, distinctive larval dentition, a rudimentary tongue, and the absence of eyelids. Larval caecilians, also smaller models of adults, have external gills, a lateral-line system (a group of epidermal sense organs located over the head and along the side of the body), and a thin skin.
In anurans, tadpoles are fishlike when they hatch. They have short, generally ovoid bodies and long, laterally compressed tails that are composed of a central axis of musculature with dorsal and ventral fins. The mouth is located terminally (recessed), ringed with an oral disk that is often fringed by papillae and bears many rows of denticles made of keratin. Tadpoles often have horny beaks. Their gills are internal and covered by an operculum. Water taken in through the mouth passes over the gills and is expelled through one or more spiracular openings on the side of an opercular chamber. Anuran larvae are microphagous and thus feed largely on bacteria and algae that coat aquatic plants and debris.
Salamander larvae usually reach full size within two to four months, although they may remain larvae for two to three years before metamorphosis occurs. Some large aquatic species, such as the hellbender (Cryptobranchus alleganiensis) and the mud puppy (Necturus maculosus), never fully metamorphose and retain larval characteristics as adults (see below heterochrony). Tadpole development varies in length between species. Some anuran species living in xeric (dry) habitats, in which ephemeral ponds may exist for only a few weeks, develop and metamorphose within two to three weeks; however, most species require at least two months. Species living in cold mountain streams or lakes often require much more time. For example, the development of the tailed frog (Ascaphus truei) takes three years to complete.
Metamorphosis
Metamorphosis entails an abrupt and thorough change in an animal’s physiology and biochemistry, with concomitant structural and behavioral modifications. These changes mark the transformation from embryo to juvenile and the completion of development. Hormones ultimately control all events of larval growth and metamorphosis, and in many instances, development is accompanied by a shift from a fully aquatic life to a semiaquatic or fully terrestrial one.
Although salamanders undergo many structural modifications, these changes are not dramatic. The skin thickens as dermal glands develop and the caudal fin is resorbed. Gills are resorbed and gill slits close as lungs develop and branchial (gill) circulation is modified. Eyelids, tongue, and a maxillary bone are formed, and teeth develop on the maxillary and parasphenoid bones. Changes that occur in caecilians—the closure of the gill slit, the degeneration of the caudal fin, and the development of a tentacle and skin glands—are also minor.
Skeletal changes are much more dramatic in anurans because tadpoles make an abrupt and radical transition to their adult form. Limbs complete their development, and the forelimbs break through the opercular wall, early in metamorphosis. The tail shrinks as it is resorbed by the body, dermal glands develop, and the skin becomes thicker. As lungs and pulmonary ventilation develop, gills and their associated blood circulation disappear. Adult mouthparts replace their degenerating larval equivalents, and hyolaryngeal structures develop. All anurans except pipids (family Pipidae) develop a tongue. In the newly differentiated digestive tract, the intestine is shortened. The eyes become larger and are structurally altered; eyelids appear. These extreme changes of anuran metamorphosis clearly demarcate the shift from an aquatic to a terrestrial mode of life. Other less obvious yet nonetheless radical modifications of the larval skull and hyobranchial apparatus (that is, the part of the skeleton that serves as base for the tongue on the floor of the mouth) occur to make room for newly developed sense organs. These modifications also facilitate the transition from larval modes of feeding and respiration to those of the adult.
During metamorphosis, the urogenital system of all amphibians is also modified. A mesonephric or opisthonephric kidney—which uses nephrons located either in the middle or at the end of the nephric ridge in the developing embryo—replaces the degenerating rudimentary pronephric kidney. This transition is linked to the shift from production of a large volume of dilute ammonia to a small amount of concentrated urea. Gonads and associated ducts also appear and begin their maturation.
Heterochrony
Neoteny, once a widely used label for the condition of sexually mature larvae, has been discontinued by biologists and replaced by the concept of heterochrony. Heterochrony refers to the change in the timing and rate of developmental events, and it is a widespread feature in amphibian evolution, particularly in salamanders. During development, a structure can begin to develop sooner (predisplacement) or later (postdisplacement) in an organism than it occurred in the ancestral species or parents. Also, a structure may continue to develop beyond the previous embryological sequence (hypermorphosis) or the developmental sequence can stop earlier than normal (progenesis or hypomorphosis). Each of these heterochronic events can produce a structurally or functionally different organism.
The classical “neotenic” salamander, the axolotl (Ambystoma mexicanum), is a paedomorphic species (that is, a species that retains aspects of its juvenile form during its adult phase); it retains its larval gills. In the mole salamander (Ambystoma talpoideum), some populations also display hypomorphic development in which the development of several larval traits to the adult condition is delayed. Since the gonads mature, a population of sexually mature salamanders with a larval morphology is produced. Heterochrony also explains the presence of larval traits in adults of the salamander families Cryptobranchidae (hellbenders) and Proteidae (olms and mud puppies).
Heterochrony is not confined to salamanders. The different sized eardrums in the American bullfrog (Lithobates catesbeianus) are examples of hypermorphism in male bullfrogs. The development of the eardrums in the male extends beyond that of the female.
Life cycle
Many amphibians have a biphasic life cycle involving aquatic eggs and larvae that metamorphose into terrestrial or semiaquatic juveniles and adults. Commonly, they deposit large numbers of eggs in water; clutches of the tiger salamander (Ambystoma tigrinum) may exceed 5,000 eggs, and large bullfrogs (L. catesbeianus) may produce clutches of 45,000 eggs. Egg size and water temperature are important factors that influence an embryo’s development time. Eggs of many anuran species laid in warm water require only one or two days to develop, whereas eggs deposited in cold mountain lakes or streams may not hatch for 30 to 40 days. The development of salamander eggs often requires more time, with hatching occurring 20 to 270 days after fertilization.
Food and feeding
Adult amphibians consume a wide variety of foods. Earthworms are the main diet of burrowing caecilians, whereas anurans and salamanders feed primarily on insects and other arthropods. Large salamanders and some large anurans eat small vertebrates, including birds and mammals. Most anurans and salamanders locate prey by sight, although some use their sense of smell. The majority of salamanders and diurnal (that is, active during daylight) terrestrial anurans are active foragers, but many other anurans employ a sit-and-wait technique. Caecilians locate their underground prey with a chemosensory tentacle and capture their quarry with a powerful bite (see chemoreception). Aquatic salamanders lunge at their prey with an open mouth and appear to drag the victim in by expanding their buccal (oral) cavity. The terrestrial lunged salamander extends its sticky tongue, which is attached anteriorly to the floor of the mouth, to ensnare a meal. In lungless salamanders, the hyobranchial apparatus is not part of the process of buccal respiration; this apparatus is modified so that it can project the tongue from the mouth. The end of the tongue is sticky to adhere to prey, and prey can be captured at distances ranging from 40 to 80 percent of the salamander’s body length.
Primitive anurans have feeding mechanisms that resemble those of the typical terrestrial salamanders. More advanced anurans employ a “lingual flip,” in which the surfaces of the retracted tongue are twisted and inverted in the fully extended tongue. The pipids, which are completely aquatic, are unique among anurans; they lack a tongue and thus must essentially drag food and water into their mouth.
Form and function:
Common features
Although the structure of the muscular, skeletal, and other anatomical systems are specifically modified for each group, amphibians are often set apart from other groups of animals by their characteristic skin, or integument, and evolutionary advances in vision and hearing.
The circulatory and respiratory systems work with the integument to provide cutaneous respiration. A broad network of cutaneous capillaries facilitates gas exchange and the diffusion of water and ions between the animal and the environment. Several species of salamanders and at least one species of frog (Barbourula kalimantanensis) are lungless. Amphibians also employ various combinations of branchial and pulmonary strategies to breathe. The buccal pump mechanism, which involves the pushing of air between the lungs and the closed mouth, is present in amphibians and some groups of fishes.
In addition to its roles in respiration and maintaining water balance, the integument of amphibians contains poison glands that release toxins. Specific toxins are found only in amphibians and are used to defend against predators.
The eye of the modern amphibian (or lissamphibian) has a lid, associated glands, and ducts. It also has muscles that allow its accommodation within or on top of the head, depth perception, and true colour vision. These adaptations are regarded as the first evolutionary improvements in vertebrate terrestrial vision. Green rods in the retina, which permit the perception of a wide range of wavelengths, are found only in lissamphibians.
The amphibian auditory system is also specially adapted. One modification is the papilla amphibiorum, a patch of sensory tissues that is sensitive to low-frequency sound. Also unique to lissamphibians is the columella-opercular complex, a pair of elements associated with the auditory capsule that transmit airborne (columella) or seismic (operculum) signals.
Structural differences
The environment helps to mold the morphology of an organism. The markedly different structural forms of the three living orders demonstrate that each group has had a long, separate evolutionary history.
Salamanders
Salamanders have less-specialized morphologies than do the other two orders. They have small heads and long slender bodies made up of four limbs and a tail. Although the skulls of most terrestrial salamanders consist of more individual pieces than do those of either caecilians or anurans, they are arched, narrow, and not well roofed. These skulls have an extra set of articulations with the vertebral column, a characteristic that may have been an evolutionary strategy for stabilizing the head on the axial skeleton (vertebral column) in terrestrial salamanders; other amphibians developed a specialized trunk musculature to meet this challenge.
The hyoid apparatus in the floor of the mouth enables salamanders to capture prey by projecting their fleshy tongues from the buccal cavity, although most are only able to roll their tongues forward over their lower jaws to snare their dinner. Food is held and manipulated in the buccal cavity by the teeth and tongue. This mechanism does not require adaptations to the mandibular and jaw muscles or sturdy, specialized teeth—features that most salamanders lack. Well-developed eyes and nasal organs, however, are needed to locate prey. Because salamanders do not depend on their vocal abilities, their auditory apparatus is less specialized than that of anurans.
Most salamander species have a generalized mode of locomotion, which is reflected by a lack of specialization in the musculoskeletal system. Salamanders walk methodically and move the limbs in the standard diagonal-sequence gait of quadrupeds. Aquatic salamanders show the greatest divergence from this generalized morphological pattern. Because they are kept afloat by their aquatic environment, they are often larger, devoid of limbs, and swim via the lateral undulation of the trunk and tail.
Caecilians
Of the three living amphibian orders, caecilians show the least divergence in structure and form. All caecilians, except for a few aquatic species, lead subterranean existences and thus have similar specialized morphologies. They have a wormlike appearance, with compact and bony heads in which the centres of ossification have fused to provide a strong, spadelike braincase. While useful in tunneling through the soil, this compact cranium does not allow much room for the jaw muscles to develop. Thus, the lower jaw is attached to the main adductor muscle of the jaw by a retroarticular process outside the cranium, and the caecilian cannot extend its tongue from the buccal cavity.
Vision, of little importance in the caecilian’s environment, is not acute; however, the nasal organs are well developed, and chemosensory perception is greatly enhanced by the existence of a tentacle (see chemoreception). The sense of hearing is probably less sensitive than that of salamanders or anurans. If the operculum (a feature analogous to auditory stapes) is present, it is incorporated into the columella (the rod made of bone or cartilage connecting the tympanic membrane with the internal ear).
Subterranean movement and feeding are aided by alterations of the axial musculoskeletal system. The overlying skin is attached to the axial muscles, and this creates a tough sheath that encases the long, muscular body and covers the posterior part of the skull. Caecilians move through soil by a process called concertina locomotion, in which the body alternately folds and extends itself along its entire length, often occurring within the envelope of skin as well as by flexures of the entire body.
Anurans
Anurans are more widespread, diverse, and numerous than either salamanders or caecilians. Anurans display a broader range of specialization in locomotion, feeding, and reproduction in their adaptation to many different environments and lifestyles. In general, anurans have a broad, flat head—which is almost as wide as their body—and a short trunk that, aside from the sacral area, is relatively inflexible. Long, powerful hind limbs propel the fused head and trunk in a forward trajectory. These leaping movements require more complex pectoral and pelvic girdles than that of salamanders. The pectoral girdle is designed to absorb the shock of the anuran as it lands on its forelimbs; an elastic, muscular suspension connecting the pectoral girdle to the skull and vertebral column provides this ability. The pelvic girdle horizontally flanks the coccyx, the bony rod at the posterior end of the vertebral column. Muscles and ligaments attach the pelvic girdle to the coccyx, sacrum, presacral vertebrae, and proximal part of the hind limb. Thus, when the animal jumps, the pelvic girdle lies in the same plane as the axial column, and, when the animal sits, the posterior end of the girdle is deflected ventrally.
In addition to the specializations for leaping, many anurans have developed structures that allow them to burrow or climb trees. These structures primarily involve modifications in limb proportions and iliosacral articulation. Arboreal (tree-dwelling) anurans have long limbs and digits with large, terminal, adhesive pads; anurans that burrow have short sturdy limbs and large spatulate tubercles made of keratin on their feet. The pipids, specialized for their aquatic environment, have little flexibility in their axial skeletons and instead propel their flat, fused bodies through the water with powerful hind limbs and large, fully webbed feet.
Anurans depend on their visual acumen for feeding and locomotion, and hence the eyes of most species are large and well developed. Because vocalizing is part of their mating and territorial behaviour, their ears are also well developed. Most species have an external tympanum (eardrum), a structure that is absent in salamanders and caecilians.
Additional Information
Amphibians are a class of cold-blooded vertebrates made up of frogs, toads, salamanders, newts, and caecilians (wormlike animals with poorly developed eyes). All amphibians spend part of their lives in water and part on land, which is how they earned their name—“amphibian” comes from a Greek word meaning “double life.” These animals are born with gills, and while some outgrow them as they transform into adults, others retain them for their entire lives.
Amphibians are the most threatened class of animals in nature. They are extremely susceptible to environmental threats because of their porous eggs and semipermeable skin. Every major threat, from climate change to pollution to disease, affects amphibians and has put them at serious risk.
Amphibians live part of their lives in water and part on land. They are vertebrates and are also ectothermic; they cannot regulate their own body heat, so they depend on sunlight to become warm and active. Amphibians also can't cool down on their own, so if they get too hot, they have to find a burrow or some other shade. In cold weather, amphibians tend to be sluggish and do not move around much.
Metamorphosis
Young amphibians do not look like their parents. Generally called larvae, they change in body shape, diet, and lifestyle as they develop, a process called metamorphosis. A frog is a good example, starting out as a tadpole with gills to breathe underwater and a tail to swim with. As the young frog gets older, it develops lungs, legs, and a different mouth. Its eyes also change position, and it loses its tail. At this point it is an adult frog and spends most of its time hopping on land rather than swimming like a fish in the water.
Moist is Best
Most amphibians have soft, moist skin that is protected by a slippery secretion of mucus. They also tend to live in moist places or near water to keep their bodies from drying out. Many adult amphibians also have poison-producing glands in their skin, which make them taste bad to predators and might even poison a predator that bites or swallows them. Some of these amphibians, like poison frogs, are brightly colored as a warning: Don't eat me, or you'll be sorry!
Three Groups
There are about 5,500 known amphibian species, divided into three main groups: salamanders and newts, caecilians, and frogs and toads. The largest amphibian is the Chinese giant salamander at nearly 6 feet (1.8 meters) and 140 pounds (63 kilograms), and the smallest is the gold frog at 0.39 inches (1 centimeter) long.

#10 This is Cool » Potassium Iodide » Yesterday 00:06:14
- Jai Ganesh
- Replies: 0
Potassium Iodide
Gist
Potassium iodide (KI) is an inorganic compound used to protect the thyroid gland from radiation, treat iodine deficiency, and manage specific skin conditions. Primarily taken as a tablet, it blocks the absorption of radioactive iodine during emergencies and serves as a supplement to combat hyperthyroidism and goiter.
Potassium iodide (KI) is a medication used to protect the thyroid gland from radiation during emergencies, treat hyperthyroidism and thyroid storm, and act as an expectorant to loosen mucus in the lungs. It is also used to treat certain fungal infections (sporotrichosis) and chronic skin conditions like erythema nodosum.
Summary
Potassium iodide (KI) is a chemical compound, medication, and dietary supplement. It is a medication used for treating hyperthyroidism, in radiation emergencies, and for protecting the thyroid gland when certain types of radiopharmaceuticals are used. It is also used for treating skin sporotrichosis and phycomycosis. It is a supplement used by people with low dietary intake of iodine. It is administered orally.
Common side effects include vomiting, diarrhea, abdominal pain, rash, and swelling of the salivary glands. Other side effects include allergic reactions, headache, goitre, and depression. While use during pregnancy may harm the baby, its use is still recommended in radiation emergencies. Potassium iodide has the chemical formula KI. Commercially it is made by mixing potassium hydroxide with iodine.
Potassium iodide has been used medically since at least 1820. It is on the World Health Organization's List of Essential Medicines. Potassium iodide is available as a generic medication and over the counter. Potassium iodide is also used for the iodization of salt.
Details
Potassium iodide (KI) is a medication that treats certain medical conditions — including some thyroid conditions — and protects your thyroid from radiation exposure. Never take KI without talking to a healthcare provider first. They’ll make sure it’s safe for you and explain proper dosing.
Overview:
What is potassium iodide?
Potassium iodide is a salt that healthcare providers sometimes use as a medication to treat certain thyroid conditions or protect your thyroid from radiation exposure.
Potassium iodide acts as a thyroid blocker, which means it stops your thyroid from releasing thyroid hormone. This can be useful in certain situations, like if your thyroid is producing high levels of thyroid hormone (hyperthyroidism). Potassium iodide can also help protect your thyroid from absorbing radioactive iodine that accidentally enters your body.
Healthcare providers intentionally use radioactive iodine — in controlled, safe amounts — for certain imaging tests and treatments. Nuclear weapon detonations and nuclear power plant accidents release unsafe amounts of radioactive iodine (radioiodine) into the air, water and soil. Potassium iodide can protect you from such unintended environmental exposure.
Potassium iodide comes in pill (tablet) and liquid forms. Some forms require a prescription, while others you can get over the counter (OTC). You should only take potassium iodide in any form if your healthcare provider or public health officials tell you to do so. Remember that just because you can buy something over the counter doesn’t mean it’s safe or appropriate for you to take.
What conditions are treated with potassium iodide?
Healthcare providers sometimes use potassium iodide to treat:
* Hyperthyroidism, particularly when associated with Graves’ disease.
* Thyroid storm.
* Some skin conditions, including cutaneous sporotrichosis (a fungal infection).
* Iodine deficiency.
Potassium iodide is also a prescription-strength expectorant. If you have a chronic lung disease, your healthcare provider may prescribe potassium iodide to loosen mucus and make it easier for you to cough.
Potassium iodide can also help protect your thyroid:
* During radiation emergencies (like a nuclear power plant meltdown).
* During medical testing (like MIBG scans) or treatments that expose your thyroid to radiation.
Potassium iodide for radiation
Potassium iodide is best known for protecting people during a radiation emergency. But it’s important to know there are limitations. Potassium iodide only protects your thyroid from radioactive iodine (one specific radioactive material). It doesn’t protect other parts of your body, and it doesn’t protect you from all the other radioactive materials you might be exposed to that could cause radiation sickness.
Healthcare providers and public health officials only recommend using potassium iodide in certain types of radiation emergencies. These typically include nuclear power plant accidents.
Potassium iodide won’t completely protect you if a nuclear bomb goes off because the greatest threat in that situation isn’t radioactive iodine. You’d be exposed to hundreds of other types of radioactive materials, and potassium iodide has no effect on those. If a bomb goes off, don’t worry about trying to find potassium iodide. Instead, seek shelter indoors and follow local officials’ guidance.
Thyroid protection after a nuclear power plant accident
Potassium iodide can help protect your thyroid from radioactive iodine released in a nuclear power plant accident. Here’s why. Your thyroid needs iodine to function normally and produce thyroid hormone. But it doesn’t know the difference between normal iodine (like what you get from your food) and radioactive iodine. This means your thyroid grabs iodine from wherever it can.
Nuclear power plant accidents may release radioactive iodine into the nearby environment. If you breathe in contaminated air or eat contaminated food, the radioactive iodine can enter your body. Your thyroid then absorbs it. Depending on the amount that gets into your body, radioactive iodine can damage your thyroid and potentially lead to thyroid cancer down the road.
The younger you are, the more vulnerable you are to the harmful effects of radioactive iodine. Babies and children face the greatest threat. If you’re pregnant, radioactive iodine is more dangerous for you compared to other adults because your thyroid is more active during pregnancy.
That’s where potassium iodide comes into play. It fills up your thyroid with enough iodine to keep it busy for a while. So, instead of absorbing the radioactive iodine, your thyroid ignores it, and the radioactive iodine passes out of your body in your pee.
Treatment Details:
How should I use potassium iodide?
Depending on your diagnosis, your healthcare provider may prescribe potassium iodide in tablet or liquid form. Your provider or local public health officials will tell you:
* How to take potassium iodide.
* When to take it.
* The appropriate dosage.
The dosage can vary widely according to the condition you’re treating. In the context of radiation emergencies, the recommended dosage varies according to a person’s age.
How long should I take potassium iodide?
It depends on the reason you’re taking it. Follow your healthcare provider’s guidance. In radiation emergencies, one dose typically protects you for about 24 hours. So, most people should take one dose per day until local officials say it’s safe to stop taking it.
Pregnant women and newborns should only take one dose (no repeat doses) unless told otherwise. That’s because potassium iodide may impact thyroid function in fetuses and newborns.
Risks / Benefits:
What are the potential benefits of potassium iodide?
When used during a radiation emergency, potassium iodide can lower a person’s risk of developing thyroid cancer down the road. This is especially important in children and adults under age 40, who face a greater risk of thyroid cancer from radioactive iodine exposure.
What are the side effects of potassium iodide?
Possible side effects of potassium iodide include:
* Skin rash.
* Swollen salivary glands.
* Metallic taste in your mouth.
* Burning of your mouth and throat.
* Sore teeth and gums.
* Upset stomach, nausea and diarrhea.
* Headache.
* Head cold symptoms, like a runny nose.
Newborns who are given more than a single dose of potassium iodide run the risk of developing hypothyroidism.
Can potassium iodide cause an allergic reaction?
Potassium iodide causes an allergic reaction in some people. Signs of an allergic reaction include:
* Fever.
* Joint pain.
* Swelling of your face, lips, tongue, throat, hands or feet.
* Wheezing and/or shortness of breath.
* Difficulty speaking or swallowing.
Call a healthcare provider right away if you develop signs of an allergic reaction. Call your local emergency number if you have trouble breathing, speaking or swallowing.
Taking more potassium iodide than healthcare providers or local officials recommend can make you very sick or even be fatal. That’s why it’s crucial to follow expert advice closely when taking potassium iodide or giving it to a child.
Is taking potassium iodide safe for me?
Potassium iodide isn’t safe for everyone. It’s important to check with your healthcare provider before taking potassium iodine to make sure it’s OK for you. In general, potassium iodine may not be safe to take if you:
* Have thyroid nodules as well as heart disease.
* Are taking certain medications, including those that affect how your thyroid works.
* Are sensitive or allergic to iodine.
* Have chronic kidney (renal) failure.
* Have tuberculosis or acute bronchitis.
* Have a history of adrenal insufficiency (Addison’s disease).
* Have a weakened immune system.
* Are pregnant or breastfeeding. In some situations, like radiation emergencies, the benefits of taking potassium iodide while pregnant or nursing may outweigh the risks. Follow your provider’s guidance closely.
Be sure to talk to your provider before starting potassium iodide or any other medicine. They’ll review your medical history and decide if it’s safe for you. They can tell you the benefits and risks of potassium iodide in your unique situation. They’ll also tell you if you need follow-ups or monitoring.
Recovery and Outlook:
Is there anything I can do to make this treatment easier on me?
Your provider may recommend taking potassium iodide along with milk or juice to limit stomach upset. Talk to your provider if you’re concerned about side effects or have a history of any medication allergies.
Additional Information
* In a radiation emergency, some people may be told to take potassium iodide (KI) to protect their thyroid.
* Do not take KI unless instructed by public health or emergency response officials or a healthcare provider.
* KI is recommended only for people under 40 and women who are pregnant or breastfeeding.
* KI can have harmful effects when used incorrectly. Only use KI products that are approved by the U.S. FDA.
Potassium iodide (KI) is a type of iodine that is not radioactive. It can be used to help block one type of radioactive material, radioactive iodine, from being absorbed by the thyroid.
In some radiation emergencies, radioactive iodine may be released into the environment and enter the body through breathing or eating. This is known as internal contamination.
The thyroid is a gland in the neck that plays an important role in many body functions. When the thyroid absorbs high levels of radioactive iodine, it can increase the risk of thyroid cancer many years after exposure in infants, children, and young adults.
How KI protects the thyroid
KI is the stable (non-radioactive) form of iodine. They are both absorbed by the thyroid.
The thyroid cannot distinguish between stable or radioactive iodine. To protect the thyroid from radioactive iodine, a person must take KI before or shortly after being exposed to radioactive iodine to saturate the thyroid and prevent the radioactive iodine from concentrating in the thyroid.
When a person takes the right amount of KI at the right time, it can help block the thyroid from absorbing radioactive iodine. This happens because the thyroid has already absorbed the KI, and there is no room to absorb the radioactive iodine. Think of filling a jar with blue marbles (KI). If you then pour green marbles (radioactive iodine) over the jar, there will not be room and they will just spill out.
Use KI only if instructed
Do not take KI unless you are instructed by public health or emergency response officials or a healthcare provider. KI can cause harmful health effects. KI is helpful only in specific situations for certain groups of people.
KI should be used only as directed.
* Do not use table salt or foods that contain iodine as a substitute for KI. They do not help prevent internal contamination, and eating large amounts could be harmful.
* Only use KI products that have been approved by the Food and Drug Administration (FDA). Dietary supplements that contain iodine may not work to protect the thyroid and can hurt you.
Important
KI can have harmful health effects and can cause allergic reactions. Only take KI if instructed by public health or emergency response officials or a healthcare provider.
Limits of KI use
KI is most effective if taken shortly before or right after internal contamination with radioactive iodine. The effectiveness of KI also depends on how much radioactive iodine gets into the body and how quickly it is absorbed in the body.
KI is only recommended for people under 40 and women who are pregnant or breastfeeding. People with certain medical conditions, including known iodine sensitivity, should not take KI or should talk to a healthcare provider about whether they can safely take KI.
KI only offers limited protection in specific situations:
* KI protects only against radioactive iodine and does not protect against other types of radioactive materials.
* KI protects only the thyroid. KI does not protect other parts of the body.
* KI must be taken within 24 hours before or 4 hours after exposure to be most effective.
* KI is not a treatment and cannot reverse damage already done to the thyroid.
* KI may not give a person 100% thyroid protection from radioactive iodine.
Most radiation emergencies will involve other types of radioactive materials and not radioactive iodine alone. Radioactive iodine is most common in nuclear power plant incidents.
How to take KI
KI is recommended as a medical countermeasure to protect the thyroid from radioactive iodine in people under 40 and women who are pregnant or breastfeeding. This is because younger people's cells are still growing and increasing in number more quickly. This puts them at risk for developing thyroid cancer after breathing in radioactive iodine.
Adults over 40 years old have a much lower risk of developing thyroid cancer. They are also more likely to have health conditions, like problems with their thyroids, that increase the risk for harmful health effects from KI. However, officials or healthcare providers may instruct adults over 40 to consume KI if the predicted exposure is high enough to cause hypothyroidism (when the thyroid does not make enough hormones).
Breastfeeding women should consider temporarily stopping breastfeeding until evacuated from the impacted area, if possible, and safely feed your baby other ways. Radioactive iodine can be passed to infants through breast milk.
There are two U.S. FDA-approved forms of KI:
* Tablets in two strengths, 130 milligram (mg) and 65 mg. The tablets may be cut into smaller pieces for lower doses.
* Oral liquid solution available in one concentration, each milliliter (mL) containing 65 mg of KI. The solution comes in a 1 oz (30 mL) bottle with a dropper marked for 1, 0.5, and 0.25 mL dosing. For reference, 5 mL of liquid is one teaspoon. One mL would be about the size of a large drop of water.
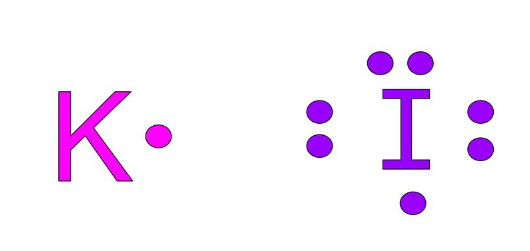
#11 Re: Dark Discussions at Cafe Infinity » crème de la crème » Yesterday 00:04:24
2467) Cecil Frank Powell
Gist:
Work
Charged particles moving through photographic emulsions leave tracks that can be examined in the images developed afterward. Cecil Powell made improvements to this technique in order to study radiation and nuclear reactions. In 1947 he discovered that incident cosmic ray particles could react with atomic nuclei in the emulsion, creating other, short-lived particles. These particles turned out to be pi-mesons, the particles proposed by Yukawa as mediating the strong force binding protons and neutrons in nuclei.
Summary
Cecil Frank Powell (born December 5, 1903, Tonbridge, Kent, England—died August 9, 1969, Casargo, Italy) was a British physicist and winner of the Nobel Prize for Physics in 1950 for his development of the photographic method of studying nuclear processes and for the resulting discovery of the pion (pi-meson), a heavy subatomic particle. The pion proved to be the hypothetical particle proposed in 1935 by Yukawa Hideki of Japan in his theory of nuclear physics.
In 1928 Powell was appointed research assistant at the Henry Herbert Wills Physical Laboratory at the University of Bristol. He became professor of physics at Bristol in 1948 and director of the Wills Laboratory in 1964. Between 1939 and 1945 he developed the necessary techniques for using sensitive photographic emulsions to record the paths of cosmic rays. In plates exposed at the top of high mountains or sent up in high-altitude balloons, cosmic-ray interactions were recorded, and in 1947 the data revealed the existence of the pion (π+) as well as the process whereby it decays into two other particles, an antimuon (mu-meson) and a neutrino. Powell also discovered the antipion (π−) and, in 1949, the modes of decay of kaons (K-mesons).
Details
Cecil Frank Powell (5 December 1903 – 9 August 1969) was a British experimental physicist who received the Nobel Prize in Physics in 1950 for heading the team that developed the photographic method of studying nuclear processes, and for the resulting discovery of the pion (pi-meson).
Education
Cecil Frank Powell was born on 5 December 1903 in Tonbridge, England, the son of Frank Powell, a gunsmith, and Elizabeth Caroline Bisacre.
Powell was educated at a local primary school before gaining a scholarship to The Judd School. He then entered Sidney Sussex College, Cambridge, graduating in 1925 with First Class Honours in the Natural Sciences Tripos. After completing his bachelor's degree, he worked under Ernest Rutherford and C. T. R. Wilson in the Cavendish Laboratory, conducting research on condensation phenomena. He received his Ph.D. in Physics in 1927.
In 1932, Powell married Isobel Artner (1907–1995). They had two daughters, Jane and Annie.
Career and research
In 1927, Powell became a research assistant to Arthur Mannering Tyndall in the H. H. Wills Physical Laboratory at the University of Bristol. He was later appointed lecturer and, in 1948, Melville Wills Professor of Physics.[6] In 1936, he took part in a Royal Society expedition to Montserrat in the West Indies as part of a study of a damaging earthquake swarm. He appears on a stamp issued in Grenada.
During his time at Bristol University, Powell applied himself to the development of techniques for measuring the mobility of positive ions, to establishing the nature of the ions in common gases, and to the construction and use of a Walton generator to study the scattering of atomic nuclei. He also began to develop methods employing specialised photographic emulsions to facilitate the recording of the tracks of elementary particles, and in 1938 began applying this technique to the study of cosmic radiation, exposing photographic plates at high-altitude, at the tops of mountains and using specially designed balloons, collaborating in the study with Giuseppe Occhialini, Hugh Muirhead, and César Lattes. This work led in 1947 to the discovery of the pion (pi-meson), which proved to be the hypothetical particle proposed in 1935 by Hideki Yukawa in his theory of nuclear forces.
In 1950, Powell was awarded the Nobel Prize in Physics "for his development of the photographic method of studying nuclear processes and his discoveries regarding mesons made with this method." Lattes was working with him at the time of the discovery and had improved the sensitivity of the photographic emulsion. Lattes was the first to write an article describing the discovery that would lead to the Nobel Prize. Debendra Mohan Bose and Bibha Chowdhuri published three consecutive papers in Nature, but could not continue further investigation on account of "non-availability of more sensitive emulsion plates" during the war years.
Seven years after this discovery of mesons by Bose and Chowdhuri, Powell made the same discovery of pions and muons and further decay of muons to electrons… using the same technique". He acknowledged in his book, "In 1941, Bose and Chaudhuri had pointed it out that it is possible, in principle, to distinguish between the tracks of protons and mesons in an emulsion… They concluded that many of the charged particles arrested in their plates were lighter than protons, their mean mass being … the physical basis of their method was correct and their work represents the first approach to the scattering method of determining momenta of charged particles by observation of their tracks in emulsion". In fact, the measured mass of the particle by Bose and Chowdhuri was very close to the accepted value measured by Powell who used improved "full-tone" plates. From 1952, Powell was appointed director of several expeditions to Sardinia and the Po Valley, Italy, utilizing high-altitude balloon flights.
In 1955, Powell, also a member of the World Federation of Scientific Workers, added his signature to the Russell–Einstein Manifesto put forward by Bertrand Russell, Albert Einstein, and Joseph Rotblat, and was involved in preparations for the first Pugwash Conference on Science and World Affairs. As Rotblat put it, "Cecil Powell has been the backbone of the Pugwash Movement. He gave it coherence, endurance and vitality." Powell chaired the meetings of the Pugwash Continuing Committee, often standing in for Bertrand Russell, and attended meetings until 1968.
In 1961, Powell served on the Scientific Policy Committee of the European Organization for Nuclear Research (CERN).
Global policy
He was one of the signatories of the agreement to convene a convention for drafting a world constitution. As a result, for the first time in human history, a World Constituent Assembly convened to draft and adopt the Constitution for the Federation of Earth.
Death
On 9 August 1969, Powell died of a heart attack while on holiday with his wife in the Valsassina region of Italy, lodging in a house in Sanico, in the Province of Lecco.
Giuseppe Occhialini had a wooden bench built with Powell's name carved into a commemorative plaque, and then transported it to Premana, a village in the mountains above Lake Como. It was installed on the path where he died, outside the Rifugio Capanna Vittoria (now the Capanna Vittoria restaurant), on the Alpe Giumello, in Casargo. Occhialini's reason was, "...if that bench had already been there, Powell would probably have stopped to rest there."

#12 Jokes » Orange Jokes - III » Yesterday 00:04:03
- Jai Ganesh
- Replies: 0
Q: Why did the orange fail his driving test?
A: He kept peeling out.
* * *
Q: How many marmalade sandwiches did Paddington bear eat?
A: None he was already stuffed.
* * *
Q: What do you call an orange that takes over the world?
A: Orange Julius Caesar.
* * *
Q: Do you now why a orange is smart?
A: Because it CONCERTRATES!
* * *
Q: What do you call the ruthless movie about building a fruit empire?
A: There Will Be Blood...Oranges.
* * *
#13 Dark Discussions at Cafe Infinity » Comfortable Quotes - III » Yesterday 00:03:41
- Jai Ganesh
- Replies: 0
Comfortable Quotes - III
1. I think the actresses who are really successful are the ones who are comfortable in their own skins and still look human. - Emma Watson
2. I love wearing whatever is comfortable, and that could be something which was in trend years ago. So, I don't follow fashion. - Virat Kohli
3. I feel fine and comfortable with myself, but not because I'm beautiful. - Monica Bellucci
4. I have been learning English on the road since I started when I was 15, so it is a slow process but making some progress. Now I think I am much more comfortable with my English. However, it is difficult, still, when I speak about something that is not tennis. - Rafael Nadal
5. It is my first preference to do films with social significance. Art cinema has given me credibility and status as an actor, but commercial cinema has given me a comfortable living. - Om Puri
6. You need to do what's comfortable to you... if it doesn't suit your personality then I wouldn't try to be someone I'm not. - Michael Clarke
7. History and experience tell us that moral progress comes not in comfortable and complacent times, but out of trial and confusion. - Gerald R. Ford
8. I meet people overseas that know five languages - that the only language I'm comfortable in is English. - Bill Gates.
#14 This is Cool » Bone Marrow » 2026-03-22 17:57:47
- Jai Ganesh
- Replies: 0
Bone Marrow
Gist
Bone marrow is the soft, spongy, and highly vascularized tissue located in the cavities of bones—primarily the pelvis, ribs, and sternum—that serves as the body's main blood cell "factory". It produces red blood cells (oxygen transport), white blood cells (immune defense), and platelets (clotting) from hematopoietic stem cells, making it essential for life.
Bone marrow is the soft, spongy, highly vascular tissue found in the center of bones, primarily acting as the body's main blood cell factory. It contains stem cells that produce essential components: red blood cells (oxygen delivery), white blood cells (immune defense), and platelets (clotting).
Summary
Bone marrow is a semi-solid tissue found within the spongy (also known as cancellous) portions of bones. In birds and mammals, bone marrow is the primary site of new blood cell production (or haematopoiesis). It is composed of hematopoietic cells, marrow adipose tissue, and supportive stromal cells. In adult humans, bone marrow is primarily located in the ribs, vertebrae, sternum, and bones of the pelvis. Bone marrow comprises approximately 5% of total body mass in healthy adult humans, such that a person weighing 73 kg (161 lbs) will have around 3.7 kg (8 lbs) of bone marrow.
Human marrow produces approximately 500 billion blood cells per day, which join the systemic circulation via permeable vasculature sinusoids within the medullary cavity. All types of hematopoietic cells, including both myeloid and lymphoid lineages, are created in bone marrow; however, lymphoid cells must migrate to other lymphoid organs (e.g. thymus) in order to complete maturation.
Bone marrow transplants can be conducted to treat severe diseases of the bone marrow, including certain forms of cancer such as leukemia. Several types of stem cells are related to bone marrow. Hematopoietic stem cells in the bone marrow can give rise to hematopoietic lineage cells, and mesenchymal stem cells, which can be isolated from the primary culture of bone marrow stroma, can give rise to bone, adipose, and cartilage tissue.
Details
Bone marrow is the soft, fatty tissue inside of the bones in your body. Bone marrow contains cells that produce blood cells and platelets and it is responsible for making billions of new blood cells each day.
Overview:
What is bone marrow?
Bone marrow is the soft, fatty tissue inside of bone cavities. Components of your blood including red and white blood cells and platelets form inside of your bone marrow.
Function:
What does bone marrow do?
Bone marrow makes nearly all the components of your blood. It's responsible for creating billions of red blood cells daily, along with white blood cells and platelets. Bone marrow also stores fat that turns into energy as needed.
Can you live without bone marrow?
Bone marrow makes the components of your blood that you need to survive. Bone marrow produces red blood cells that carry oxygen, white blood cells that prevent infection and platelets that control bleeding. The absence of bone marrow can be fatal since it's an essential part of your body.
Can I donate bone marrow?
Yes, bone marrow and the healthy cells it produces are necessary for humans to live. Often, cell mutations harm healthy bone marrow cells, and a bone marrow transplant would be a treatment option for people diagnosed with blood cancers like leukemia.
A bone marrow transplant takes healthy cells from a donor and puts them into your bloodstream. The donor’s cells help your body grow healthy red and white blood cells and platelets.
Anatomy:
Where is bone marrow located?
There are three parts to the anatomy of your bones: compact bone, spongy bone and bone marrow. Compact bone is the strong, outer layer of your bones. Spongy bone makes up the ends of your bones. Bone marrow is in the center of most bones and in the end of spongy bones in your body. Bone marrow and blood vessels fill cavities in your bones, where they store fat and stem cells and produce blood cells that make your whole blood.
What does bone marrow look like?
Bone marrow is a spongy, soft tissue that resembles a jelly or jam that you would spread on toast. It comes in two colors, red and yellow. Bone marrow fills the cavities of your bones and holds cells that create red and white blood cells and platelets, which make whole blood. The color of red bone marrow is the result of red blood cell production.
What are the two types of bone marrow?
There are two types of bone marrow in your body, which are characterized by their color. Your body holds just under 6 lbs. (about 2.5 kg.) of red and yellow bone marrow.
* Red: Red bone marrow produces blood cells (hematopoiesis). Stem cells in your red bone marrow (hematopoietic stem cells) create red and white blood cells and platelets, all of which are components of your whole blood.
* Yellow: Yellow bone marrow stores fat. There are two types of stem cells in yellow bone marrow (adipocytes and mesenchymal stem cells). These cells preserve fat for energy production and develop bone, cartilage, muscles and fat cells for your body.
Red bone marrow makes up all of your bone marrow until about age seven. Yellow bone marrow gradually replaces red bone marrow as you age.
What is bone marrow made of?
Bone marrow is made of stem cells. These stem cells make red bone marrow, which creates blood cells and platelets for your blood. Yellow bone marrow consists mostly of fat and stem cells that produce bone and cartilage in your body.
Conditions and Disorders:
What are common conditions and disorders that affect bone marrow?
Directly targeting bone marrow is leukemia, which is a blood and bone marrow cancer. Leukemia forms when a cell mutation occurs in your bone marrow and mutated cells multiply out of control, reducing the production of healthy, normal cells.
Since bone marrow is the foundation for the creation of blood cells, blood-related conditions often are the result of abnormally functioning bone marrow. These conditions include:
* Multiple myeloma: Your body produces cancerous plasma cells in your bone marrow.
* Aplastic anemia: Your bone marrow doesn’t produce enough blood cells.
* Polycythemia vera: Your body makes too many red blood cells, which causes your blood to thicken.
* Myelodysplastic syndromes: A group of diseases characterized by your bone marrow not producing enough healthy blood cells (anemia).
What are common symptoms of bone marrow conditions?
Common symptoms of bone marrow conditions include:
* Bleeding easily,
* Bruising.
* Fatigue.
* Frequent infections.
* Muscle weakness.
What are common tests to check the health of my bone marrow?
There are two tests to check the health of your bone marrow and/or blood cells:
* Bone marrow aspiration: A needle removes fluid and cells from your bone marrow (bone marrow concentrate). The aspirate test identifies what cells are present in your bone marrow, verifies whether or not those cells are normal or abnormal and gives other information about the characteristics of your cells.
* Bone marrow biopsy: A large needle removes a piece of your bone marrow. The biopsy shows where, how many and the types of cells are present in your bone marrow.
Is it painful to remove my bone marrow?
For a bone marrow test or donation, you’ll receive an anesthetic, so you won't feel any pain during the procedure. After the procedure, you may feel side effects, which include aches and pain at the site of the incision. Each individual experiences pain differently, so the severity could vary from person to person. The pain may last for a few days or up to several weeks.
What are common treatments for bone marrow conditions?
Treatments for bone marrow conditions vary based on the severity and progress of the diagnosis. Treatment options include:
* Antibiotics.
* Blood transfusions.
* Bone marrow transplant.
* Chemotherapy.
* Supportive care to relieve symptoms.
* Stem cell transplant.
Care:
How do I keep my bone marrow healthy?
Bone marrow is the foundation of your bones, blood and muscles. Keeping your bone marrow healthy focuses on supporting components of your body that grow from bone marrow cells. You can keep your bone marrow healthy by:
* Eating a diet rich in protein (lean meats, fish, beans, nuts, milk, eggs).
* Taking vitamins (iron, B9, B12).
* Treating medical conditions where bone marrow abnormalities are a side effect.
Additional Information
Bone marrow is a soft, gelatinous tissue that fills the cavities of the bones. Bone marrow is either red or yellow, depending upon the preponderance of hematopoietic (red) or fatty (yellow) tissue. In humans the red bone marrow forms all of the blood cells with the exception of the lymphocytes, which are produced in the marrow and reach their mature form in the lymphoid organs. Red bone marrow also contributes, along with the liver and spleen, to the destruction of old red blood cells. Yellow bone marrow serves primarily as a storehouse for fats but may be converted to red marrow under certain conditions, such as severe blood loss or fever. At birth and until about the age of seven, all human marrow is red, as the need for new blood formation is high. Thereafter, fat tissue gradually replaces the red marrow, which in adults is found only in the vertebrae, hips, breastbone, ribs, and skull and at the ends of the long bones of the arm and leg; other cancellous, or spongy, bones and the central cavities of the long bones are filled with yellow marrow.
Red marrow consists of a delicate, highly vascular fibrous tissue containing stem cells, which differentiate into various blood cells. Stem cells first become precursors, or blast cells, of various kinds; normoblasts give rise to the red blood cells (erythrocytes), and myeloblasts become the granulocytes, a type of white blood cell (leukocyte). Platelets, small blood cell fragments involved in clotting, form from giant marrow cells called megakaryocytes. The new blood cells are released into the sinusoids, large thin-walled vessels that drain into the veins of the bone. In mammals, blood formation in adults takes place predominantly in the marrow. In lower vertebrates a number of other tissues may also produce blood cells, including the liver and the spleen.
Because the white blood cells produced in the bone marrow are involved in the body’s immune defenses, marrow transplants have been used to treat certain types of immune deficiency and hematological disorders, especially leukemia. The sensitivity of marrow to damage by radiation therapy and some anticancer drugs accounts for the tendency of these treatments to impair immunity and blood production.
Examination of the bone marrow is helpful in diagnosing certain diseases, especially those related to blood and blood-forming organs, because it provides information on iron stores and blood production. Bone marrow aspiration, the direct removal of a small amount (about 1 ml) of bone marrow, is accomplished by suction through a hollow needle. The needle is usually inserted into the hip or sternum (breastbone) in adults and into the upper part of the tibia (the larger bone of the lower leg) in children. The necessity for a bone marrow aspiration is ordinarily based on previous blood studies and is particularly useful in providing information on various stages of immature blood cells. Disorders in which bone marrow examination is of special diagnostic value include leukemia, multiple myeloma, Gaucher disease, unusual cases of anemia, and other hematological diseases.
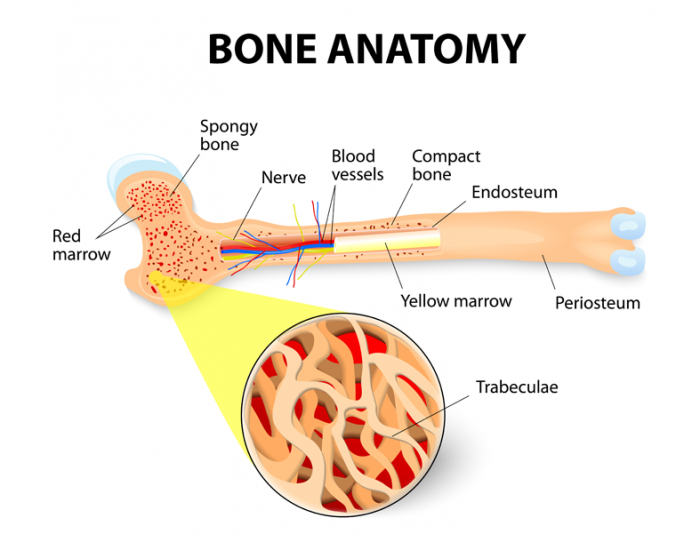
#15 Science HQ » Jaundice » 2026-03-22 17:22:06
- Jai Ganesh
- Replies: 0
Jaundice
Gist
Jaundice is the yellowing of the skin and eyes caused by excess bilirubin in the blood, signaling underlying liver dysfunction, bile duct obstruction, or accelerated red blood cell destruction. Common causes include hepatitis, cirrhosis, gallstones, and, in newborns, immature liver function.
Jaundice is primarily caused by a buildup of bilirubin in the blood, resulting from liver dysfunction, bile duct obstruction, or rapid red blood cell breakdown. Common underlying factors include hepatitis, liver cirrhosis, gallstones, alcohol-related liver disease, and pancreatic cancer, which prevent proper processing or excretion of bilirubin.
Summary
Jaundice, also known as icterus, is a yellowish or, less frequently, greenish pigmentation of the skin and sclera due to high bilirubin levels. Jaundice in adults typically indicates the presence of underlying diseases involving abnormal heme metabolism, liver dysfunction, or biliary-tract obstruction. The prevalence of jaundice in adults is rare, while jaundice in babies is common, with an estimated 80% affected during their first week of life. The most commonly associated symptoms of jaundice are itchiness,[2] pale feces, and dark urine.
Normal levels of bilirubin in blood are below 1.0 mg/dl (17 μmol/L), while levels over 2–3 mg/dl (34–51 μmol/L) typically result in jaundice. High blood bilirubin is divided into two types: unconjugated and conjugated bilirubin.
Causes of jaundice vary from relatively benign to potentially fatal. High unconjugated bilirubin may be due to excess red blood cell breakdown, large bruises, genetic conditions such as Gilbert's syndrome, not eating for a prolonged period of time, newborn jaundice, or thyroid problems. High conjugated bilirubin may be due to liver diseases such as cirrhosis or hepatitis, infections, medications, or blockage of the bile duct, due to factors including gallstones, cancer, or pancreatitis. Other conditions can also cause yellowish skin, but are not jaundice, including carotenemia, which can develop from eating large amounts of foods containing carotene—or medications such as rifampin.
Treatment of jaundice is typically determined by the underlying cause. If a bile duct blockage is present, surgery is typically required; otherwise, management is medical. Medical management may involve treating infectious causes and stopping medication that could be contributing to the jaundice. Jaundice in newborns may be treated with phototherapy or exchanged transfusion depending on age and prematurity when the bilirubin is greater than 4–21 mg/dl (68–365 μmol/L). The itchiness may be helped by draining the gallbladder, ursodeoxycholic acid, or opioid antagonists such as naltrexone. The word jaundice is from the French jaunisse, meaning 'yellow disease'.
Details
Jaundice is a condition where your skin, the whites of your eyes and mucous membranes (like the inside of your nose and mouth) turn yellow. Many medical conditions can cause jaundice, like hepatitis, gallstones and tumors. Jaundice usually clears up once your healthcare provider treats your main medical condition.
Overview:
What is jaundice?
Jaundice (hyperbilirubinemia) is when your skin, sclera (whites of your eyes) and mucous membranes turn yellow. Jaundice occurs when your liver is unable to process bilirubin (a yellow substance made when red blood cells break down) in your blood. This can either be caused by too much red blood cell breakdown or liver injury.
How jaundice develops:
* Red blood cell breakdown: Your body regularly breaks down old red blood cells and replaces them with new ones. This breakdown process makes bilirubin.
* Bilirubin processing: Normally, your liver processes bilirubin, making it a part of bile (a bitter, greenish-brown fluid that helps digest food). Your liver then releases the bile into your digestive system.
* Too much bilirubin: Jaundice happens when your liver can’t process all the bilirubin your body makes, or if your liver has a problem releasing bilirubin.
* Yellow color: When there’s too much bilirubin in your blood, it starts to leak into tissues around your blood vessels. This leaking bilirubin makes your skin and the whites of your eyes yellow. This yellow color is a common sign of jaundice.
Possible Causes:
What causes jaundice?
Jaundice can result from a problem in any of the three phases of bilirubin:
* Before your liver processes bilirubin (prehepatic jaundice). This type of jaundice happens before your body makes bilirubin. Too much red blood cell breakdown takes over your liver’s ability to filter out bilirubin from your blood.
* During the production of bilirubin (hepatic jaundice). This type happens when your liver can’t remove enough bilirubin from your blood. Hepatic jaundice can happen if you have liver failure.
* After production of bilirubin (posthepatic jaundice). Also called obstructive jaundice, this type happens when a blockage stops bilirubin from draining into your bile ducts.
Conditions that cause jaundice include:
Prehepatic jaundice causes
* Breaking down a large hematoma (bruise) and then reabsorbing it back into your bloodstream.
* Hemolytic anemias (when blood cells are destroyed and removed from the bloodstream before their normal lifespan is over).
Hepatic jaundice causes
* Viruses, including hepatitis A, chronic hepatitis B and C, and Epstein-Barr virus infection (infectious mononucleosis).
* Alcohol-induced hepatitis.
* Autoimmune disorders.
* Rare genetic metabolic defects.
* Medicines, including penicillin, oral contraceptives, chlorpromazine (Thorazine R), estrogenic or anabolic steroids and acetaminophen toxicity.
Posthepatic jaundice causes
* Gallstones.
* Inflammation (swelling) of your gallbladder.
* Gallbladder cancer.
* Pancreatic tumor.
How do you know if you have jaundice?
You may not notice the yellow skin and sclera associated with jaundice. Your provider may find the condition when looking for something else. How serious your symptoms are depends on what causes them and how quickly or slowly they develop.
Symptoms that can be associated with jaundice include:
* Yellowish tint to your skin and the whites of your eyes.
* Fever.
* Chills.
* Pain in your belly.
* Flu-like symptoms.
* Dark-colored pee.
* Pale-colored poop.
* Being tired or confused.
* Itchy skin.
* Weight loss.
Care and Treatment:
How can my provider tell I have jaundice?
Your provider can tell if you have jaundice by measuring the bilirubin levels in your blood and seeing whether it’s the type of bilirubin related to red blood cell breakdown (unconjugated) or liver injury (conjugated). They may also check for other signs of liver disease, including:
* Bruising.
* Spider angiomas (abnormal collection of blood vessels near the surface of your skin).
* Palmar erythema (red palms and fingertips).
Your healthcare provider will also examine you to decide your liver’s size and tenderness. They may use imaging (ultrasound and CT scanning) and liver biopsy (taking a tissue sample of your liver) to better understand what’s causing your liver injury.
How is jaundice treated?
There’s no specific treatment for jaundice. But your provider can treat the cause and the jaundice should improve. They can also treat complications the condition causes. For example, if itchy skin is a problem, your provider can prescribe medication.
What are the risks of not treating jaundice?
It depends on what’s causing your jaundice. If it’s a virus, the virus could spread or become chronic. But if you have jaundice because your liver is failing, complications from your liver disease can include coma and death.
Can you prevent jaundice?
Since there are many causes of jaundice, it’s hard to find ways to prevent it. Some general tips include:
* Avoiding hepatitis infection by getting vaccinated, having safe sex, using clean needles and practicing good personal hygiene like thorough hand-washing with soap and water.
* Staying within recommended alcohol limits.
* Maintaining a weight that’s healthy for you.
* Avoiding natural and herbal supplements.
* Managing your cholesterol.
When To Call the Doctor:
When should jaundice be treated by a doctor or healthcare provider?
A healthcare provider should evaluate jaundice. It’s a sign that something’s not right with your liver. If you notice signs of jaundice, call your healthcare provider.
Additional Common Questions:
Do children get jaundice?
Jaundice is common in newborn babies. Like with adults, a buildup of bilirubin in your baby’s blood can cause jaundice. Since your baby’s liver is still developing, it can’t remove (or break down) all the bilirubin. Jaundice usually goes away on its own or providers treat it with phototherapy.
Additional Information:
What Is Jaundice?
When red blood cells die, they leave behind bilirubin, a yellow-orange pigment in the blood. The liver filters bilirubin from the bloodstream to be removed in your stool. If too much is in your system or your liver is overloaded, it causes a buildup known as hyperbilirubinemia. This causes jaundice, where your skin and the whites of your eyes look yellow.
Newborn babies often get it. About 60% have jaundice, also known as icterus, within the first couple of days after birth. Adults can get it, too, although it's less common. See a doctor right away if you think you have jaundice. It could be a symptom of a liver, blood, or gallbladder problem.
Types of Jaundice
There are four main types of jaundice, which are grouped by where the bilirubin collects in your body. A blood test can determine which type you have.
Prehepatic
If bilirubin builds up before blood enters the liver, it's known as prehepatic jaundice. This means you're breaking down red blood cells and creating more bilirubin than your liver can process.
Hepatic
If your liver isn't able to process bilirubin well, it's called hepatic jaundice.
Posthepatic
Posthepatic jaundice is when bilirubin builds up after passing through the liver and your body can't clear it quickly enough.
Obstructive jaundice
This condition is when bile isn't able to drain into your intestines because of a blocked or narrow bile or pancreatic duct. This type of jaundice has a high death rate, so it's important to catch and treat it early.
Jaundice Symptoms
Jaundice may have no symptoms. Any signs you have may depend on how quickly the condition is getting worse. Well-known symptoms are yellowing of the skin and jaundice eyes (also called scleral icterus). But there are others to watch for, including:
* Fever
* Stomach pain
* Chills
* Dark urine
* Tar- or clay-colored stools
* Flu-like symptoms
* Itchy skin
* Weight loss
* Feeling unusually irritated
* Confusion
* Abnormal drowsiness
* Bruising or bleeding easily
* Bloody vomit
How long does jaundice last in adults?
How long jaundice lasts depends on what's causing it and the treatment you need. If a medication is causing it, jaundice will fade after you stop taking it. If hepatitis is causing it, medications can be taken to treat the condition. If there is a blocked bile duct or gallstones, surgery may be required.
Jaundice Causes
Jaundice in adults is rare, but you can get it for many reasons. These include:
* Hepatitis: Liver inflammation can be caused by a virus, autoimmune disorder, alcohol or drug use, or chemical exposure. It may be short-lived (acute) or chronic, which means it lasts for at least 6 months. Long-term inflammation can damage the liver, causing jaundice.
* Alcohol-related liver disease: If you drink heavily over a long period of time – typically 8 to 10 years – you could seriously damage your liver. Two diseases in particular, alcoholic hepatitis and alcoholic cirrhosis, harm the liver.
* Other liver disease: Cirrhosis can also be caused by autoimmune diseases, genetic conditions that are passed down in your family, and hepatitis. A severe condition known as nonalcoholic steatohepatitis can cause nonalcoholic fatty liver disease. With this kind of liver disease, fat builds up in your liver along with inflammation, which damages it over time.
* Blocked bile ducts: These are thin tubes that carry a fluid called bile from your liver and gallbladder to your small intestine. If the tubes are blocked by gallstones, cancer, inflammation, or rare liver diseases, you could get jaundice.
* Pancreatic cancer: This is the 10th most common cancer in men and the ninth in women. It can block the bile duct, causing jaundice.
* Certain medicines: Drugs like acetaminophen, penicillin, birth control pills, and steroids have been linked to liver disease.
* Blood clots: If your body reabsorbs a large blot clot (hematoma) under the skin, it can increase bilirubin levels.
* Hemolytic anemias: Destroyed blood cells are sometimes removed from the bloodstream too quickly, increasing bilirubin levels.
Diagnosing Jaundice
Your doctor will ask you about your symptoms and medical history. They'll then give you a physical exam to see if there's swelling in your liver.
To get more information, your doctor will likely order blood tests to measure bilirubin and cholesterol levels and get a complete blood count (CBC). If you have jaundice, your level of bilirubin will be high. Your doctor may order other tests to find the cause of your jaundice and how severe it is, including:
* A hepatitis panel, which is a blood test that shows if you have, or have had, hepatitis. It tests for hepatitis A, hepatitis B, and hepatitis C. If there are no hepatitis antibodies in your blood, it means you don't have the condition, or you had it in the past, but your body has cleared it.
* Tests to check enzyme levels in the liver to see how well it is functioning. If enzyme levels are higher or lower than normal, it can mean you have disease or damage to the liver or bile ducts.
* Imaging, like a CT scan, ultrasound, or magnetic resonance cholangiopancreatography, a type of MRI that checks for blocked ducts near the gallbladder
* A liver biopsy, to show if you have damage to, or disease in, your liver. During the test, a small piece of your liver is removed either with a needle inserted into the belly to the liver, through a vein in your neck, or through a cut in your belly.
* Prothrombin time, which measures how long it takes for blood plasma to clot. Your blood will be taken, and a laboratory will test it to see if it clots faster or slower than the normal range (which is between 10 and 13 seconds). If it clots too slowly, that may mean there are problems with your liver.
Jaundice Treatment
In adults, jaundice itself usually isn’t treated. But your doctor will treat the condition that’s causing it.
If you have acute viral hepatitis, jaundice will go away on its own as your liver heals. If a blocked bile duct is to blame, your doctor may suggest surgery to open it. If your skin is itching, your doctor can prescribe cholestyramine to be taken by mouth. This medication is used to remove bile acids from your body, which cause itching.
Phototherapy for jaundice
Phototherapy uses a fluorescent white or blue-spectrum light that breaks down bilirubin so it can be released from the body. This treatment is used for newborns, but phototherapy has not been shown to be effective for treating jaundice in adults.
Preventing Jaundice
You may have a higher risk for jaundice if you drink too much alcohol or have hepatitis. It is also more common in people during middle age.
You can reduce your risk of jaundice through lifestyle changes like:
* Avoid herbal supplements (which can be toxic to the liver) unless recommended by your doctor
* Stop smoking
* Reduce or cut out all alcohol (the CDC recommends no more than two alcoholic drinks per day for men and one daily for women)
* Don't use intravenous drugs (drugs that go into your vein)
* Don't take more prescription medication than you are prescribed
* Get all recommended vaccines before traveling overseas
* Use safe sex practices
* Maintain a healthy weight
* Keep your cholesterol in a healthy range

#16 Re: Jai Ganesh's Puzzles » General Quiz » 2026-03-22 16:13:51
Hi,
#10807. What does the term in Geography Dike mean?
#10808. What does the term in Geography Discharge (hydrology) mean?
#17 Re: Jai Ganesh's Puzzles » English language puzzles » 2026-03-22 15:54:14
Hi,
#6013. What does the noun loyalist mean?
#6014. What does the noun lubricant mean?
#18 Re: Jai Ganesh's Puzzles » Doc, Doc! » 2026-03-22 15:41:38
#2603. What does the medical term Probenecid mean?
#19 Re: Jai Ganesh's Puzzles » 10 second questions » 2026-03-22 15:27:30
Hi,
#9889.
#20 Re: Jai Ganesh's Puzzles » Oral puzzles » 2026-03-22 15:17:23
Hi,
#6382.
#21 Re: Exercises » Compute the solution: » 2026-03-22 14:45:04
Hi,
2743.
#22 This is Cool » Iguazu Falls » 2026-03-22 00:58:58
- Jai Ganesh
- Replies: 0
Gist
Iguazu Falls is the world's largest waterfall system, featuring 275 individual cascades stretching nearly 3 kilometers along the Argentina-Brazil border. As a UNESCO World Heritage site and one of the new seven natural wonders, it features the dramatic 80-meter-tall "Devil's Throat" (Garganta del Diablo).
Iguazu Falls exists within a protected UNESCO World Heritage site that's home to over 2,000 species of vascular plants and countless animal species, including jaguars, ocelots, and over 400 bird species.
Iguazu Falls is one of the new seven natural wonders of the world. At over 1.5 miles wide it is wider than Niagara Falls and is 60% taller than Niagara Falls.
Summary
“My poor Niagara …”
That is what Eleonor Roosevelt said when she saw Iguazu Falls.
Welcome to Iguazu Falls! One of the most important destinations in Argentina, Brazil and South America!
Every year, millions of people come to visit this beautiful natural attraction that Argentina and Brazil have to offer. During 2019, the park received 1,640,000 visitors, both local and foreign.
And everyone is amazed with this destination!
The Iguazu Falls consists of two national parks, one in Foz de Iguazu (Brazil) and the other one in Puerto Iguazu (Argentina). The curious thing is that although one only sees the falls as the main attraction, the park has a size of 252,982 hectares (67,720 on the Argentine side and 185,262 on the Brazilian side).
These falls in Argentina and Brazil managed to attract so much attention that almost at the same time they were declared National Parks (1934 in Argentina and 1939 in Brazil). And after some years and millions of visitors fascinated by the landscape and the sound of this natural attraction, UNESCO declared them as World Heritage Site in 1984, and reaffirmed as Exceptional Universal Value (their cultural and nature it’s so important that it’s conservation should be of worldwide interest) in 2013.
Why are they so famous? It is enough to just see photos and videos to be amazed by its beauty. But it is not only about tourism: the Iguazu National Park is home to many species of animals and flora that create an important natural ecosystem connected to all Latin America.
Each visitor who comes to the Iguazu Falls collaborates to continue the conservation work for the area.
And obviously, Iguazu Falls have allowed the development of local economies, making the city of Puerto Iguazu and Foz de Iguazu grow and improve the quality of life of its inhabitants.
Location of Iguazu Falls
Iguazu Falls are in the continent of South America, and as we mentioned, it is shared by two countries: Argentina and Brazil. Although Paraguay is nearby, it only shares the river that Iguazu Falls feeds, but it is quite far from the falls and cannot even be seen from there.
The city in Argentina where the Iguazu Falls are located is called Puerto Iguazu, and in Brazil it is called Foz de Iguazu. Both cities are very close to each other: only 16km from center to center.
Iguazu Falls on the Argentine side are located 18km from Puerto Iguazu and 29km from the center of Foz de Iguazu.
Iguazu Falls on the Brazilian side are 27km from Puerto Iguazu, and 29km from downtown Foz de Iguazu
Both cities are very close to each national park, that is why all the excursions that we offer on both sides of the falls can pick up from any hotel in both destinations (except in hotels far from the center such as Recanto Cataratas).
The destination is close to several major cities with direct flights. For example, going to Iguazu Falls from Buenos Aires only needs to take a plane to get there in about 2 hours. From Rio de Janeiro you can also get to Iguazu in two hours.
The Iguazu Falls on the Argentine side is at latitude -25.68352837588661 and longitude -54.4547103472097.
The Iguazu Falls on the Brazilian side is at latitude -25.61524025766296 and longitude -54.479225906855845.
Airports Near Iguazu Falls
As the Iguazu Falls are shared by Argentina and Brazil, you have two airports to choose from where to get there: Puerto Iguazu (airport code IGR) and Foz de Iguazu (airport code IGU).
Getting to one or the other airport depends on where you come from to visit the destination.
If you want to visit Iguazu from destinations in Argentina such as Buenos Aires, Cordoba, Salta or other, you should look for flights arriving in Puerto Iguazu (airport code IGR).
Now if you come from Rio de Janeiro, Sao Paulo, or even some international destination like Lima (Peru), then look for flights that arrive at Foz de Iguazu (airport code IGU).
Both airports are fairly close to Iguazu Falls, in fact it is quite normal to offer one-day tours that visit the park on flights that arrive and depart the same day – although it may seem rushed, it is an excellent option for passengers who come from cruise ships or who have very little time.
Iguazu Falls on the Argentine side are 9km (15-20 minutes by car). And the falls on the Brazilian side are 4 kilometers away (less than 10 minutes by car).
Details
Iguazú Falls or Iguaçu Falls are waterfalls of the Iguazu River on the border of the Argentine province of Misiones and the Brazilian state of Paraná. Together, they make up the largest waterfall system in the world. The falls divide the river into the upper and lower Iguazu. The Iguazu River rises near the heart of the city of Curitiba. For most of its course, the river flows through Brazil; however, most of the falls are on the Argentine side. Below its confluence with the San Antonio River, the Iguazu River forms the border between Argentina and Brazil.
The name Iguazú comes from the Guarani or Tupi words y, meaning 'water', and ûasú [waˈsu], meaning 'big'. Legend has it that a deity planned to marry a beautiful woman named Naipí, who fled with her mortal lover Tarobá in a canoe. In a rage, the deity sliced the river, creating the waterfalls and condemning the lovers to an eternal fall. The first European to record the existence of the falls was the Spanish Conquistador Álvar Núñez Cabeza de Vaca in 1541. It was inscribed into the UNESCO World Heritage List in 2013.
Geology and geography
The staircase character of the falls consists of a two-step waterfall formed by three layers of basalt. The steps are 35 and 40 metres (115 and 131 ft) in height. The columnar basalt rock sequences are part of the 1,000-metre-thick (3,300 ft) Serra Geral formation within the Paleozoic-Mesozoic Paraná Basin. The tops of these sequences are characterized by 8–10 m (26–33 ft) of highly resistant vesicular basalt and the contact between these layers controls the shape of the falls. Headwater erosion rates are estimated at 1.4–2.1 cm/year (0.55–0.83 in/year). Numerous islands along the 2.7-kilometre-long (1.7 mi) edge divide the falls into many separate waterfalls and cataracts, varying between 60 and 82 m (197 and 269 ft) high. The number of these smaller waterfalls fluctuates from 150 to 300, depending on the water level. About half of the river's flow falls into a long and narrow chasm called the Devil's Throat (Garganta del Diablo in Spanish or Garganta do Diabo in Portuguese).
The Devil's Throat canyon is 80–90 m (260–300 ft) wide and 70–80 m (230–260 ft) deep. Left of this canyon, another part of the river forms 160–200 individual falls, which merge into a single front during the flood stage. The largest falls are named San Martín, Adam and Eva, Penoni, and Bergano.
About 900 m (2,950 ft) of the 2.7 km (1.7 mi) length does not have water flowing over it. The water of the lower Iguazu collects in a canyon that drains into the Paraná River, a short distance downstream from the Itaipu Dam. The junction of the water flows marks the border between Brazil, Argentina, and Paraguay. Some points in the cities of Foz do Iguaçu, Brazil, Puerto Iguazú, Argentina, and Ciudad del Este, Paraguay, have access to the Iguazu River, where the borders of all three nations may be seen, a popular tourist attraction for visitors to the three cities.
The layout of Iguazu Falls resembles a reversed letter "J". The Argentina–Brazil border runs through the Devil's Throat. On the right bank is the Brazilian territory, which is home to more than 95% of the Iguazu River basin but has just over 20% of the jumps of these falls, and the left side jumps are Argentine, which make up almost 80% of the falls.
Access
The falls may be reached from two main towns, with one on either side of the falls: Foz do Iguaçu in Brazil and Puerto Iguazú in Argentina, as well as from Ciudad del Este, Paraguay, on the other side of the Paraná River from Foz do Iguaçu, each of those three cities having commercial airports. The falls are shared by the Iguazú National Park (Argentina) and Iguaçu National Park (Brazil). The two parks were designated UNESCO World Heritage Sites in 1984 and 1986, respectively.
The first proposal for a Brazilian national park aimed at providing a pristine environment to "future generations", just as "it had been created by God" and endowed with "all possible preservation, from the beautiful to the sublime, from the picturesque to the awesome" and "an unmatched flora" located in the "magnificent Iguaçu waterfalls". These were the words used by André Rebouças, an engineer, in his book Provinces of Paraná, Railways to Mato Grosso and Bolivia, which started up the campaign aimed at preserving the Iguaçu Falls in 1876. At this time, Yellowstone National Park in the US, the first national park in the world, was four years old.
On the Brazilian side, a walkway along the canyon has an extension to the lower base of Devil's Throat. Helicopter rides offering aerial views of the falls have been available from Brazil, but Argentina has prohibited such helicopter tours because of the adverse environmental impact on the flora and fauna of the falls.
Aerolíneas Argentinas has direct flights from Buenos Aires to Iguazu International Airport. Azul, GOL, and LATAM Brasil offer services from main Brazilian cities to Foz do Iguaçu. From Foz do Iguaçu airport, the park may be reached by taking a taxi or bus to the entrance of the park. Their park has an entrance fee on both sides. Once inside, free and frequent buses are provided to various points within the park. The town of Foz do Iguaçu is about 20 km (12 mi) away, and the airport is between the park and the town.
The Argentine access, across the forest, is by a Rainforest Ecological Train very similar to the one in Disney's Animal Kingdom. The train brings visitors to the entrance of Devil's Throat, as well as the upper and lower trails. The Paseo Garganta del Diablo is a 1 km-long (0.6 mi) trail that brings visitors directly over the falls of Devil's Throat, the highest and deepest of the falls. Other walkways allow access to the elongated stretch of falls across the forest on the Argentine side and to the boats that connect to San Martin Island. Also on the Argentine side, inflatable boat services take visitors very close to the falls.
The Brazilian transportation system aims at allowing an increase in the number of visitors, while reducing the adverse environmental impact, through an increase in the average number of passengers per vehicle inside the park. The new transportation system has a 72-passenger capacity and panoramic-view, double-deck buses.
Comparison with other notable falls
Upon seeing Iguazu, the United States First Lady Eleanor Roosevelt reportedly exclaimed, "Poor Niagara!" (which, at 50 m or 165 feet, are a third shorter). Often, Iguazu also is compared with Victoria Falls in Southern Africa, which separates Zambia and Zimbabwe. Iguazu is wider but is split into roughly 275 distinct falls and large islands, whereas Victoria has the largest curtain of water in the world, at more than 1,600 m (5,249 ft) wide and over 100 m (328 ft) in height (in low flow, Victoria is split into five by islands but in high flow, it may be uninterrupted). The only wider falls are extremely large rapid-like falls, such as the Boyoma Falls (Stanley Falls).
With the flooding of the Guaíra Falls in 1982, Iguazu currently has the sixth-greatest average annual flow of any waterfall in the world, following number five Niagara, with an average rate of 1,746 {m}^{3}/s (61,660 cu ft/s). Its maximum recorded flow was 45,700 {m}^{3}/s (1,614,000 cu ft/s) on 9 June 2014. By comparison, the average flow of Niagara Falls is 2,400 {m}^{3}/s (85,000 cu ft/s), with a maximum recorded flow of 8,300 {m}^{3}/s (293,000 cu ft/s). The average flow at Victoria Falls is 1,088 {m}^{3}/s (38,420 cu ft/s), with a maximum recorded flow of 7,100 {m}^{3}/s (250,000 cu ft/s).
Climate
The Iguazu Falls experience a humid subtropical climate (Cfa, according to the Köppen climate classification) with abundant precipitation and high temperatures year-round. During the summer of 2006, a severe drought caused the Iguazu River to become diminished, reducing the amount of water flowing over the falls to 300 cubic metres per second (11,000 cu ft/s) until early December. This was unusual, as dry periods normally last only a few weeks. The period with the greatest volume of water flowing over the falls is usually December to February, coinciding with one of the periods of greatest rainfall.
Additional Information
Iguazu Falls, Iguazú Falls, Iguassu Falls, or Iguaçu Falls (Spanish: Cataratas del Iguazú [kataˈɾatas ðel iɣwaˈsu]; Guarani: Chororo Yguasu [ɕoɾoɾo ɨɣʷasu]; Portuguese: Cataratas do Iguaçu [kataˈɾatɐʒ du iɡwaˈsu]) are waterfalls of the Iguazu River on the border of the Argentine province of Misiones and the Brazilian state of Paraná. They are the largest waterfalls system in the world. The falls divide the river into the upper and lower Iguazu. The Iguazu River rises near the city of Curitiba. For most of its course, the river flows through Brazil, however, most of the falls are on the Argentine side. Below its confluence with the San Antonio River, the Iguazu River forms the boundary between Argentina and Brazil.
The name “Iguazu” comes from the Guarani or Tupi words “y”, meaning “water”, and “ûasú “[waˈsu], meaning “big”. Legend has it that a deity planned to marry a beautiful woman named Naipí, who fled with her mortal lover Tarobá in a canoe. In a rage, the deity sliced the river, creating the waterfalls and condemning the lovers to an eternal fall. The first European to record the existence of the falls was the Spanish conquistador Álvar Núñez Cabeza de Vaca in 1541.
Iguaçu Falls is a series of cataracts on the Iguaçu River, 14 miles (23 km) above its confluence with the Alto (Upper) Paraná River, at the Argentina-Brazil border. The falls resemble an elongated horseshoe that extends for 1.7 miles (2.7 km)—nearly three times wider than Niagara Falls in North America and significantly greater than the width of Victoria Falls in Africa. Numerous rocky and wooded islands on the edge of the escarpment over which the Iguaçu River plunges divide the falls into some 275 separate waterfalls or cataracts, varying between 200 and 269 feet (60 and 82 metres) in height. The name of the falls, like that of the river, is derived from a Guaraní word meaning “great water.”
The rate of flow of the falls may rise to a maximum of 450,000 cubic feet (12,750 cubic metres) per second during the rainy season from November to March. Minimum flow occurs during the dry season from August to October. The mean annual rate of flow is about 62,000 cubic feet (1,756 cubic metres) per second.
The falls occur along a wide span where the Iguaçu River, flowing westward and then northward, tumbles over the edge of the Paraná Plateau before continuing its course in a canyon. Above the falls, islands and islets spread the river into numerous flows that feed the cataracts. A major portion of the river tumbles into a narrow, semicircular chasm called the Garganta do Diabo (Spanish: Garganta del Diablo [“Devil’s Throat”]); the effect has been described as that of “an ocean plunging into an abyss.” Excellent views of this section (also called Union Falls) can be obtained from both the Brazilian and Argentine sides. Many of the individual falls are broken midway by protruding ledges; the resultant deflection of the water, as well as the spray that arises, creates an array of rainbows. From the foot of the Garganta do Diabo, a curtain of mist rises some 500 feet (150 metres) into the air.
Among the many islands along the falls, the most notable is Isla Grande San Martín, which is situated downstream from the Garganta do Diabo (on the Argentine side). From this island, a fine view of many of the cataracts may be had. Individual falls to be seen from the forest paths and trails on the Argentine side include those known as Dos Hermanas (“Two Sisters”), Bozzetti, San Martín, Escondido (“Hidden”), and Rivadavia. From the Brazilian shore, an impressive panorama of falls can also be seen; among individual Brazilian falls are those known as Benjamin Constant, Deodoro, and Floriano.
The first Spanish explorer to visit the falls was Álvar Núñez Cabeza de Vaca in 1541. In 1897 Edmundo de Barros, a Brazilian army officer, envisaged the establishment of a national park at Iguaçu Falls. Following boundary rectifications between Brazil and Argentina, two separate national parks were established, one by each country—Iguaçu National Park (1939) in Brazil and Iguazú National Park (1934) in Argentina. Both parks were created to preserve the vegetation, wildlife, and scenic beauty associated with the falls. In 1984 the Argentine park was designated a UNESCO World Heritage site, and two years later the Brazilian park was also granted World Heritage status. The Iguaçu area is served by three airports, in Argentina, Brazil, and Paraguay.
The vegetation of the region is rich and varied, ranging from semi-deciduous to tropical, and has been a focus of botanical interest. Water plants include a family (Podostemaceae) that grows only in rushing water and is found on the ledges of the falls. Contrasts are also abundant, with orchids growing next to pines, bamboos next to palm trees, and mosses next to lianas and colourful begonias.
Animal life is equally varied and abundant but has been much less studied. Iguanas are a common sight. Among the mammals are several members of the cat family (ocelots and jaguars), deer, tapir, and innumerable smaller animals. Toucans and birds of many other varieties are also to be found. Fish include the dorado (golden salmon), mandi, and cascudo.

#23 Re: This is Cool » Miscellany » 2026-03-22 00:05:24
2529) Vanadium Pentoxide
Gist
Vanadium pentoxide (V2O5) is a brownish-yellow solid inorganic compound, appearing as an orange powder when freshly precipitated. It is a crucial industrial catalyst, most notably used in the contact process to produce sulfuric acid. It serves as a strong oxidizing agent, a flux in ceramics, and a precursor to vanadium alloys and batteries.
Vanadium pentoxide (V2O5) is a crucial industrial compound primarily used as a catalyst in sulfuric acid production (contact process) and for manufacturing vanadium alloys/steel. It is also essential as a cathode material in lithium-ion and redox flow batteries, and as a coloring agent in ceramics and glass.
Summary:
Key Industrial and Technical Uses
1) Catalyst in Chemical Synthesis: V2O5 acts as a catalyst in the production of sulfuric acid, which is one of the world’s largest industrial chemicals. It is also used to produce maleic anhydride and as an oxidizer in organic chemical manufacturing.
2) Metallurgy and Alloying: Approximately 85% of total vanadium is used in special steel production, and V2O5 is the key precursor to producing vanadium aluminum master alloys for aerospace and high-stress structural applications.
3) Energy Storage (Batteries): It is a crucial component in vanadium redox flow batteries (VRFBs) for large-scale grid energy storage, as well as a cathode material in high-capacity lithium-ion batteries.
4) Ceramics and Glass Manufacturing: It is used as a pigment, yielding yellow, green, and blue colors in glazes for tiles and sanitary ware, and in specialized glass coating.
5) Other Applications: It is utilized in the manufacturing of photographic developers and as a sensing material in infrared detectors and gas sensors.
V2O5 is a highly stable metal-oxide semiconductor often used as a pigment or specialized catalytic agent in ceramic production. It is also utilized in research regarding chemical and battery applications, serving as a primary ingredient for creating higher-capacity anodes in, for instance, Sodium-Ion or Zinc-Ion battery systems.
Details
Vanadium(V) oxide (vanadia) is the inorganic compound with the formula V2O5. Commonly known as vanadium pentoxide, it is a dark yellow solid, although when freshly precipitated from aqueous solution, its colour is deep orange. Because of its high oxidation state, it is both an amphoteric oxide and an oxidizing agent. From the industrial perspective, it is the most important compound of vanadium, being the principal precursor to alloys of vanadium and is a widely used industrial catalyst.
The mineral form of this compound, shcherbinaite, is extremely rare, almost always found among fumaroles. A mineral trihydrate, V2O5·3H2O, is also known under the name of navajoite.
Preparation
Technical grade V2O5 is produced as a black powder used for the production of vanadium metal and ferrovanadium. A vanadium ore or vanadium-rich residue is treated with sodium carbonate and an ammonium salt to produce sodium metavanadate, NaVO3. This material is then acidified to pH 2–3 using H2SO4 to yield a precipitate of "red cake". The red cake is then melted at 690 °C to produce the crude V2O5.
Vanadium(V) oxide is produced when vanadium metal is heated with excess oxygen, but this product is contaminated with other, lower oxides. A more satisfactory laboratory preparation involves the decomposition of ammonium metavanadate at 500–550 °C:
2 NH4VO3 → V2O5 + 2 NH3 + H2O
Uses:
Ferrovanadium production
In terms of quantity, the dominant use for vanadium(V) oxide is in the production of ferrovanadium (see above). The oxide is heated with scrap iron and ferrosilicon, with lime added to form a calcium silicate slag. Aluminium may also be used, producing the iron-vanadium alloy along with alumina as a byproduct.
Sulfuric acid production
Another important use of vanadium(V) oxide is in the manufacture of sulfuric acid, an important industrial chemical with an annual worldwide production of 165 million tonnes in 2001, with an approximate value of US$8 billion. Vanadium(V) oxide serves the crucial purpose of catalysing the mildly exothermic oxidation of sulfur dioxide to sulfur trioxide by air in the contact process:
2 SO2 + O2 ⇌ 2 SO3
The discovery of this simple reaction, for which V2O5 is the most effective catalyst, allowed sulfuric acid to become the cheap commodity chemical it is today. The reaction is performed between 400 and 620 °C; below 400 °C the V2O5 is inactive as a catalyst, and above 620 °C it begins to break down. Since it is known that V2O5 can be reduced to VO2 by SO2, one likely catalytic cycle is as follows:
SO2 + V2O5 → SO3 + 2 VO2
followed by
2 VO2 + 1⁄2 O2 → V2O5
It is also used as catalyst in the selective catalytic reduction (SCR) of NOx emissions in some power plants and diesel engines. Due to its effectiveness in converting sulfur dioxide into sulfur trioxide, and thereby sulfuric acid, special care must be taken with the operating temperatures and placement of a power plant's SCR unit when firing sulfur-containing fuels.
Other applications
Due to its high coefficient of thermal resistance, vanadium(V) oxide finds use as a detector material in bolometers and microbolometer arrays for thermal imaging. It also finds application as an ethanol sensor in ppm levels (up to 0.1 ppm).
Vanadium redox batteries are a type of flow battery used for energy storage, including large power facilities such as wind farms. Vanadium oxide is also used as a cathode in lithium-ion batteries.
Vanadium pentoxide is often used as a component in glazes where it produces a wide range of colours from greens and yellows to blues and grays.
Additional Information
Vanadium pentoxide is used in different, industrial processes as catalyst: In the contact process it serves for the oxidation of SO2 to SO3 with oxygen at 440°C. Besides it is used in the oxidation of ethanol to ethanale and in the production of phthalic anydride, polyamide, oxalic acid and further products.
Vanadium pentoxide is a stable oxide of vanadium with an oxidation state of +5. It is extensively used as an n-type semiconductor, a cathode material in lithium batteries, and an industrial catalyst. It is also used in glass and ceramic glazes, as a steel additive, and in welding electrode coatings. Additionally, it is used as a catalyst in chemical reactions and in the manufacture of ceramics.
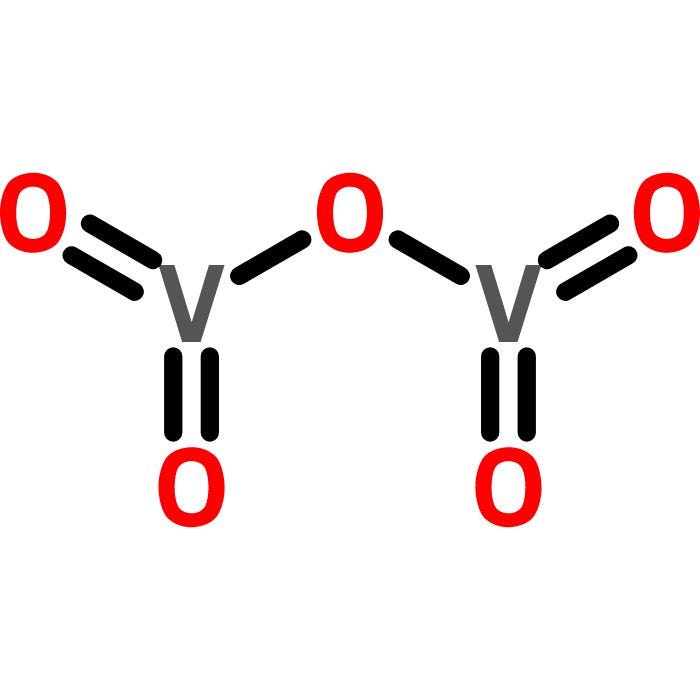
#24 Re: Dark Discussions at Cafe Infinity » crème de la crème » 2026-03-22 00:04:56
2466) Max Theiler
Gist:
Work
Yellow fever is a disease that used to be fairly common and claimed many lives in the tropics. The disease is caused by a virus and is transmitted to people by insects and also from one person to another. Max Theiler succeeded in transmitting the virus to mice, which paved the way for more in-depth research. When the virus was transmitted between mice, a weakened form of the virus was obtained that could make apes immune. In 1937 Theiler succeeded in obtaining an even weaker variant of the virus. This variant, 17D, came to be used as a human vaccine.
Summary
Max Theiler (born January 30, 1899, Pretoria, South Africa—died August 11, 1972, New Haven, Connecticut, U.S.) was a South African-born American microbiologist who won the 1951 Nobel Prize for Physiology or Medicine for his development of a vaccine against yellow fever.
Theiler received his medical training at St. Thomas’s Hospital, London, and the London School of Hygiene and Tropical Medicine, graduating in 1922. In that year he joined the department of tropical medicine at Harvard Medical School, Boston. There he carried out important studies of amebic dysentery and rat-bite fever and began work on yellow fever.
In 1930 Theiler joined the laboratories at the Rockefeller Foundation’s International Health Division in New York City, where he continued his research on infectious diseases, including yellow fever. With the discovery in 1928 that rhesus monkeys were susceptible to the virus responsible for yellow fever, researchers began to develop vaccines against the disease. Theiler discovered that the common mouse is also susceptible to the yellow fever virus, a finding that facilitated the vaccine research. In the late 1930s Theiler developed the first attenuated, or weakened, strain of the virus. Further studies led to the development of the improved 17D strain that became widely used for human immunization against yellow fever.
Theiler was director of the Rockefeller Foundation Virus Laboratories from 1951 to 1963. After retiring from the Rockefeller Foundation in 1964, he became professor of epidemiology and microbiology at Yale University, where he remained until 1967.
Details
Max Theiler (30 January 1899 – 11 August 1972) was a South African-American virologist and physician. He was awarded the Nobel Prize in Physiology or Medicine in 1951 for developing a vaccine against yellow fever in 1937, becoming the first African-born Nobel laureate.
Born in Pretoria, Theiler was educated in South Africa through completion of his degree in medical school. He went to London for postgraduate work at St Thomas's Hospital Medical School and at the London School of Hygiene and Tropical Medicine, earning a 1922 diploma in tropical medicine and hygiene. That year, he moved to the United States to do research at the Harvard University School of Tropical Medicine. He lived and worked in that nation the rest of his life. In 1930, he moved to the Rockefeller Foundation in New York, becoming director of the Virus Laboratory.
Early life and education
Theiler was born in Pretoria, the capital of the South African Republic (now South Africa); his father Arnold Theiler was a veterinary bacteriologist. He attended Pretoria Boys High School, Rhodes University College, and University of Cape Town Medical School, graduating in 1918. He left South Africa for London to study at St Thomas's Hospital Medical School, King's College London, and at the London School of Hygiene and Tropical Medicine. In 1922, he was awarded a diploma in tropical medicine and hygiene; he became a licentiate of the Royal College of Physicians of London and a member of the Royal College of Surgeons of England.
Career development
Theiler wanted to pursue a career in research, so in 1922, he took a position at the Harvard University School of Tropical Medicine in Cambridge, Massachusetts. He spent several years investigating amoebic dysentery and trying to develop a vaccine for rat-bite fever.
After becoming assistant to Andrew Sellards, he started working on yellow fever. In 1926, they disproved Hideyo Noguchi's hypothesis that yellow fever was caused by the bacterium Leptospira icteroides. In 1928, the year after the disease was identified conclusively as being caused by a virus, they showed that the African and South American viruses are immunologically identical. (This followed Adrian Stokes' inducing yellow fever in rhesus macaques from India). In the course of this research, Theiler contracted yellow fever, but survived and developed immunity.
In 1930, Theiler moved to the Rockefeller Foundation in New York, where he later became director of the Virus Laboratory. He was professor of epidemiology and public health at the Yale School of Medicine and the School of Public Health from 1964 to 1967.
Work on yellow fever
After passing the yellow fever virus through laboratory mice, Theiler found that the weakened virus conferred immunity on rhesus macaques. The stage was set for Theiler to develop a vaccine against the disease. Theiler first devised a test for the efficacy of experimental vaccines. In his test, sera from vaccinated human subjects were injected into mice to see if they protected the mice against yellow fever virus. This "mouse protection test" was used with variations as a measure of immunity until after World War II. Subculturing the particularly virulent Asibi strain from West Africa in chicken embryos, a technique pioneered by Ernest Goodpasture, the Rockefeller team sought to obtain an attenuated strain of the virus that would not kill mice when injected into their brains. It took until 1937, and more than 100 subcultures in chicken embryos, for Theiler and his colleague Hugh Smith to obtain an attenuated strain, which they named "17D". Animal tests showed the attenuated 17D mutant was safe and immunizing. Theiler's team rapidly completed the development of a 17D vaccine, and the Rockefeller Foundation began human trials in South America. Between 1940 and 1947, the Rockefeller Foundation produced more than 28 million doses of the vaccine and finally ended yellow fever as a major disease.
For this work, Theiler received the 1951 Nobel Prize in Physiology or Medicine. Theiler also was awarded the Royal Society of Tropical Medicine and Hygiene's Chalmers Medal in 1939, Harvard University's Flattery Medal in 1945, and the American Public Health Association's Lasker Award in 1949.
Theiler's murine encephalomyelitis virus
In 1937, Max Theiler discovered a filterable agent that was a known cause for paralysis in mice. He found the virus was not transmittable to rhesus macaques (rhesus monkey, a species of Old World Monkey) and that only some mice developed symptoms. The virus is now referred to as Theiler's murine encephalomyelitis virus. The virus has been well characterized, and now serves as a standard model for studying multiple sclerosis.
Private life
He married Lillian Graham (1895–1977) in 1928, and they had one daughter. He died on 11 August 1972 in New Haven, Connecticut.

#25 Jokes » Orange Jokes - II » 2026-03-22 00:04:38
- Jai Ganesh
- Replies: 0
Q: What did the apple say to the orange?
A: Nothing stupid, apples don't talk.
* * *
Q: Why do the Tennessee Volunteers have orange jerseys?
A: So they can play the game, direct traffic, and pick up trash without changing.
* * *
Q: Where do plastic oranges live?
A: Orange County.
* * *
Q: Why did the orange go to the doctor?
A: It wasn't peeling well.
* * *
Q: What kind of monkey doesn't eat bananas?
A: An orangutan.
* * *